Articles Shoulder Dislocations
Nature has designed your shoulders for movement so that you can scratch the middle of your back, reach up high and out to the side. Unfortunately, this amazing range of movement comes at a cost. Shoulder dislocations are common and the most frequently displaced joint in the human body!

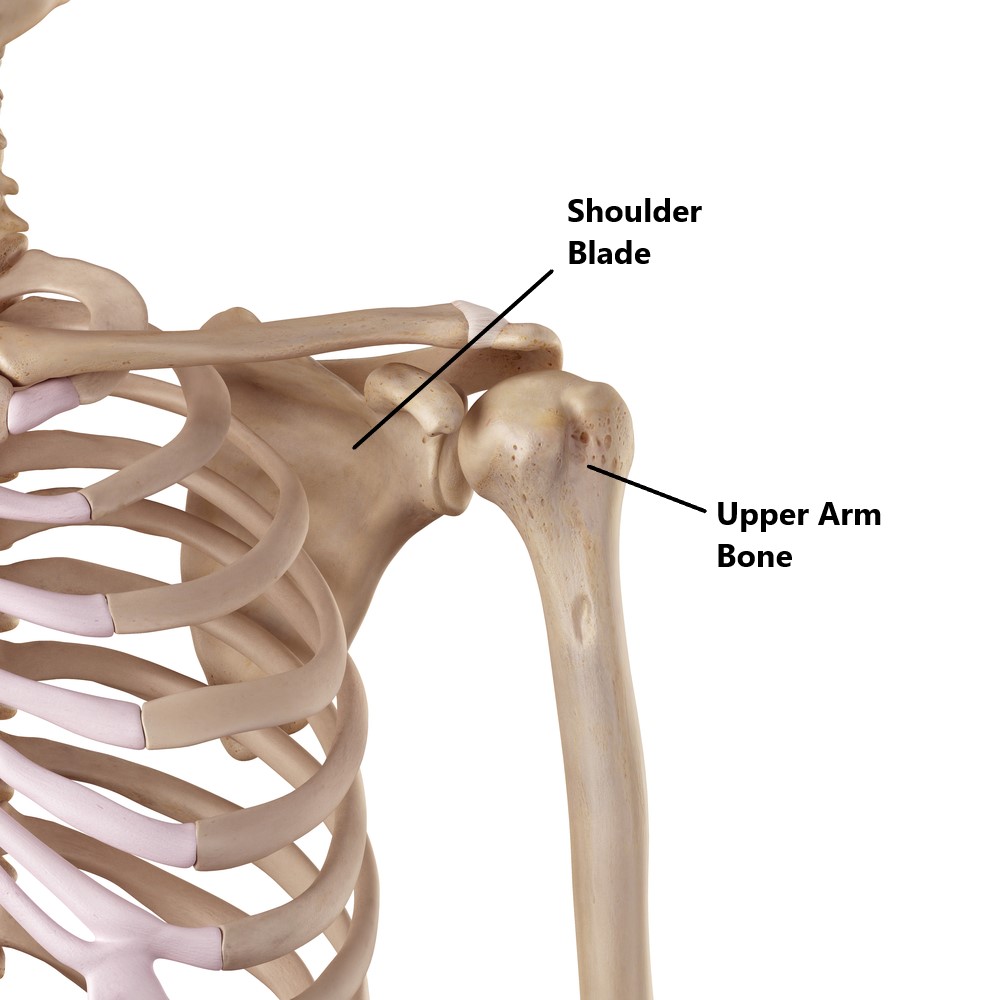
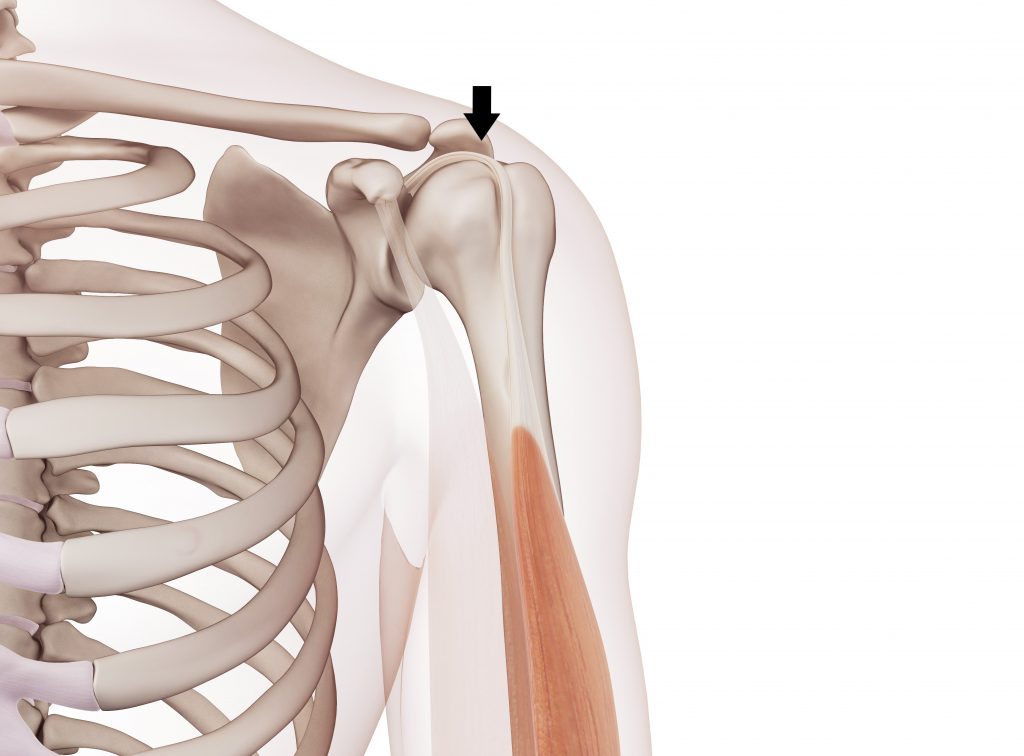
Basic Anatomy
Your shoulder is comprised of the upper arm bone and shoulder blade. These bones connect to form a shallow ball and socket joint much like a golf ball sitting on a tee. This articulation is very unstable and your body relies heavily on the surrounding structures provide stability.
What are the Stabilising Structures of the Shoulder Joint?
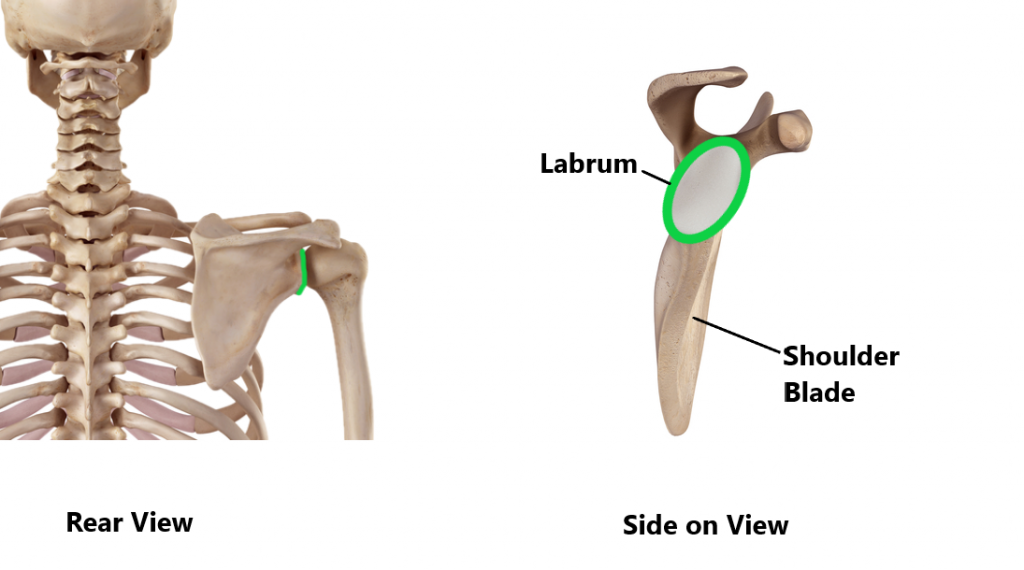
Labrum
A ring of cartilage called the labrum is located around the rim of the socket. This helps to provide additional stability by increasing the depth of the golf tee.
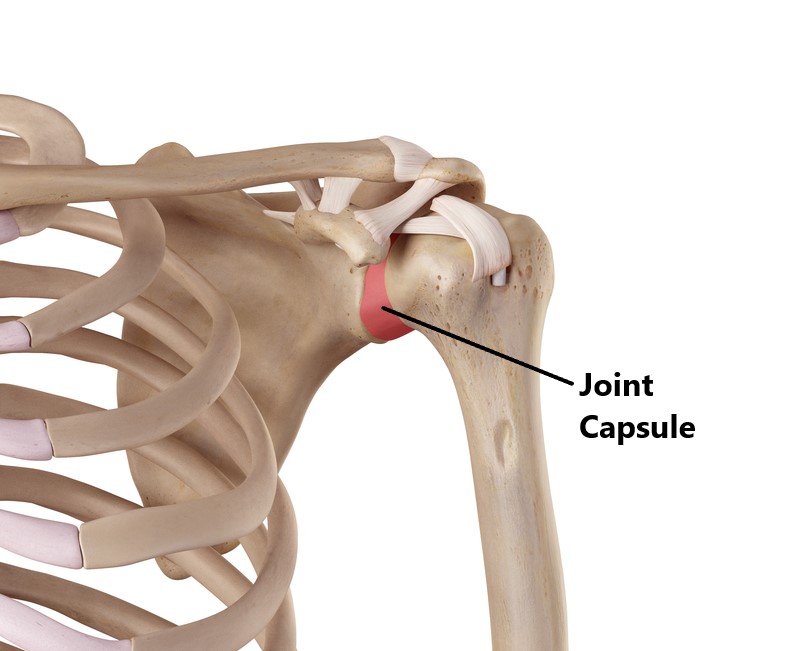
Joint Capsule and Ligaments
Connecting the ball to the socket is a strong joint capsule. Thickenings at the top, front and bottom of the joint capsule form the ligaments. These prevent excessive movement between the ball and socket.
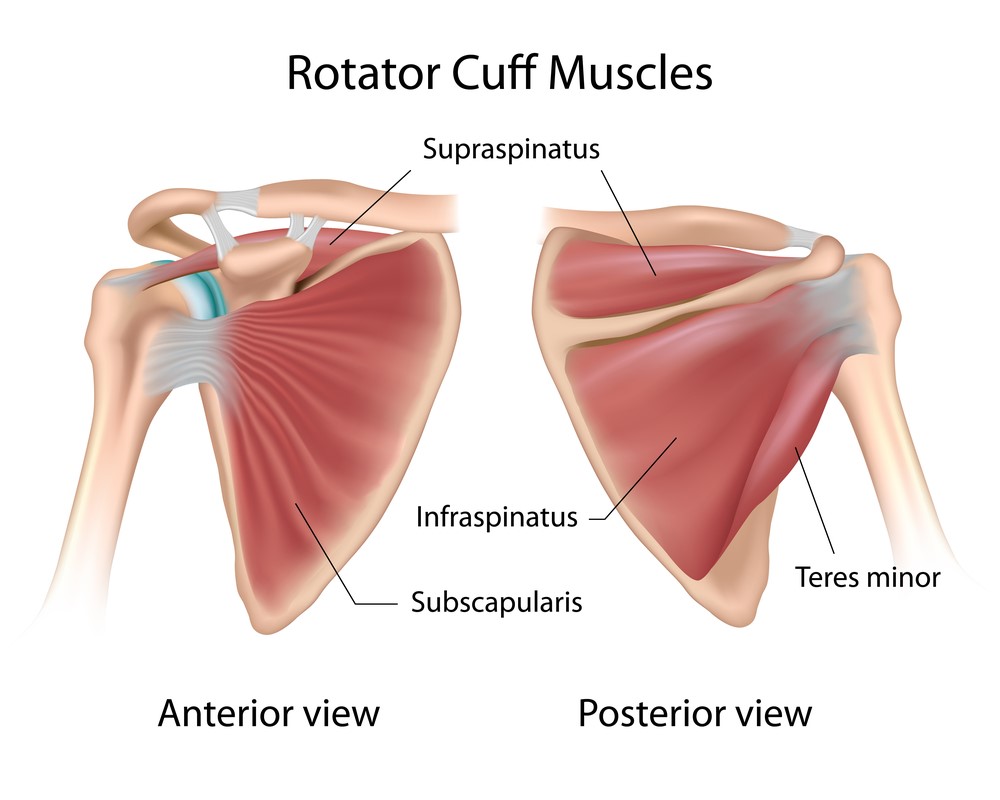
Rotator Cuff
Your rotator cuff is a group of 4 muscles. The muscle bellies arise from the shoulder blade and their tendons all attach onto the ball of the shoulder. Their primary role is to keep the “golf ball” centred on the “tee” while the shoulder moves through range.
Long Head of Biceps Tendon (LHB)
The LHB tendon assists the rotator cuff by resisting upwards translation of the “golf ball”.
Types of Shoulder Dislocations:
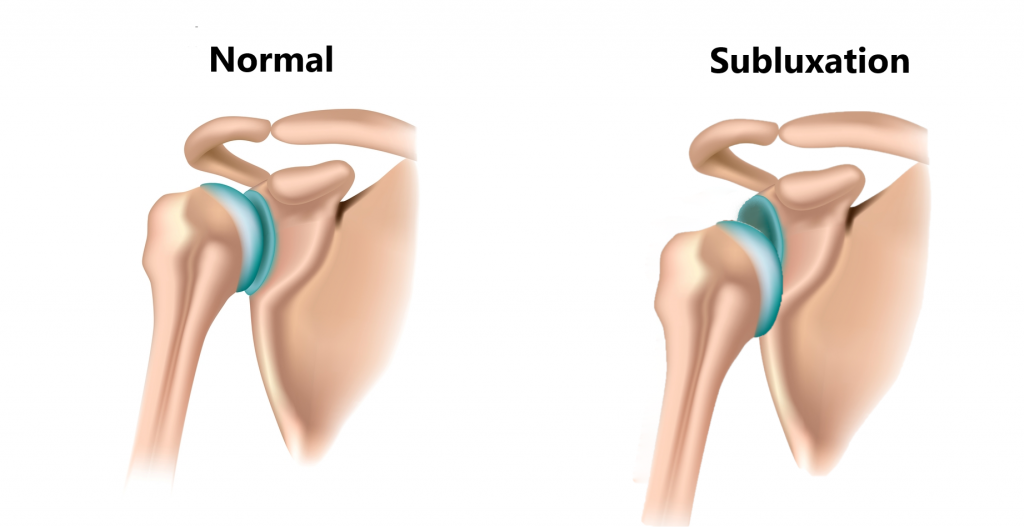
Subluxations
These are partial dislocations where the ball is not completely displaced out of the socket. Repeated subluxations can eventually lead to a full dislocation.
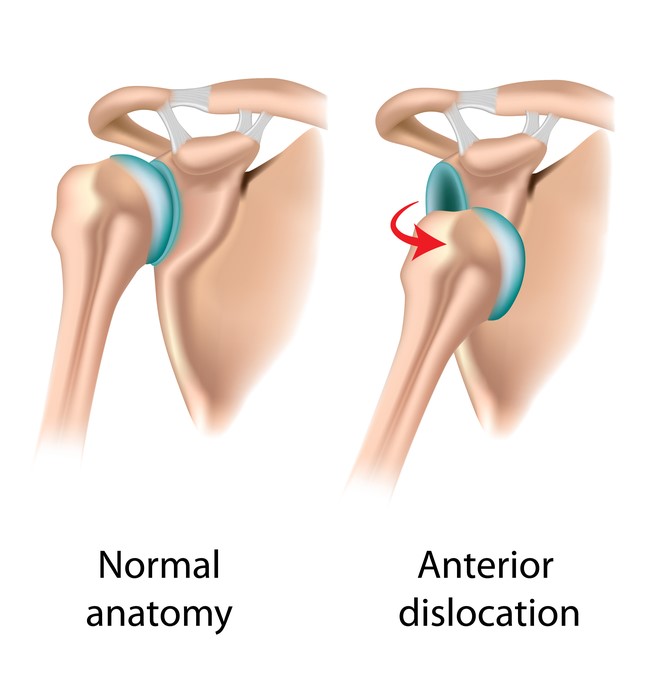
Anterior Dislocations
These injuries account for approximately 97% of all shoulder dislocations. In these situations the ball of the shoulder is displaced forwards relative to the position of the socket.
Anterior dislocations can be caused by:
- Acute trauma, these normally occur when the arm in a “stop sing” position while the hand is forced backwards (i.e. breaking a fall with your hands above your head). This is your shoulder’s most unstable position where the ligaments at the front of your joint are fully stretched. Much like a rubber band, it will only stretch to a certain point before it starts to tear.

- Overuse, These are typically seen in people who engage in overhead sports (i.e. baseball, volley ball). The late cocking stage of the throwing motion places your shoulder into the very same position as described above. Repeated strain and over use can lead to over stretching of the ligaments and eventually a joint dislocation.

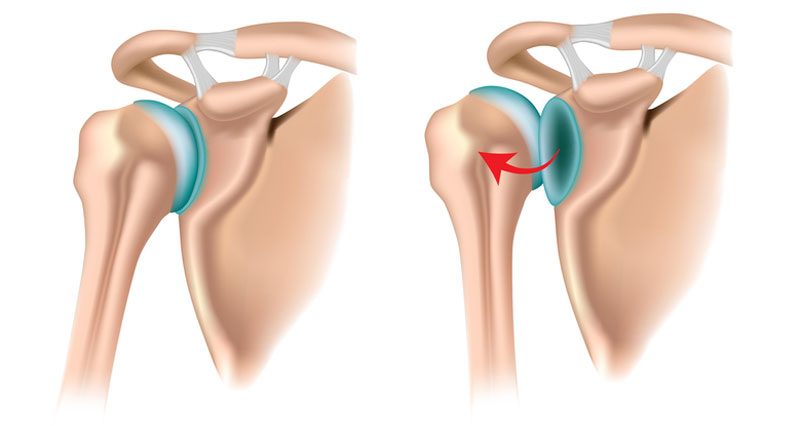
Posterior Dislocation
Posterior dislocations are far less common (approximately 3%) and are often misdiagnosed. In these situations the ball of the shoulder is displaced backwards relative to the position of the socket.
These are typically caused by acute trauma rather than overuse. Causes can include:
- following a forceful impact through the hand/elbow while the arm is raised to shoulder height (i.e. car accident while holding on to the steering wheel, fall onto elbow)
- following a forceful blow to the front of the shoulder (i.e. hard shoulder charge)
- violent muscle contraction of the posterior shoulder muscles following a seizure or electrocution

Multi Directional Instability
In this condition the shoulder joint is unstable in multiple directions (rather than one specific direction), making you more prone to dislocations. The causes do not normally involve acute trauma and can be due to:
- Joint Hypermobility, some individuals are born with naturally loose ligaments through out their entire body making them more prone to joint dislocations.

- Overuse, this is typically seen in overhead athletes (i.e. swimmers, tennis players). Repeated strain can gradually loosen the ligaments of the shoulder joint in multiple directions.

Rotator Cuff Weakness/Paralysis
This is most apparent in people who have suffered a stroke where they loose the muscle tone to the rotator cuff. The “centering function (as described above) of the cuff is lost resulting in multi directional instability.
Recurrence Rate of Shoulder Dislocations
Following a dislocation your ligaments never fully recover and become looser. The risk of recurrence is highest in young active males. It has been estimated you have an 80% chance of re-dislocating your shoulder if you are a male in your 20s! At the other end of the spectrum, people who are >50 years of age only have a 20% change of re-dislocation.

Associated Injuries with Shoulder Dislocations
Due to the high level of trauma required to dislocate your shoulder, more often than not there will be damage to the surrounding structures. Unfortunately, this increases your risk of requiring surgery.
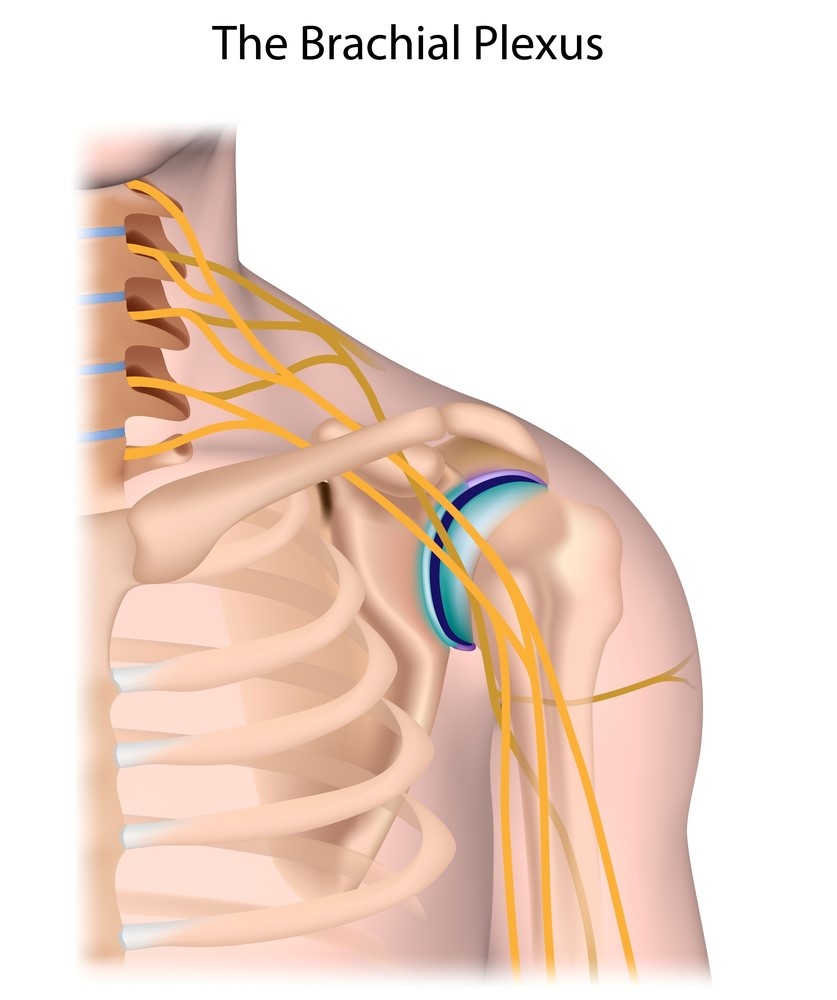
Nerve Injury
A network of nerves arising from the neck and shoulder are susceptible to traction injuries. This can give rise to symptoms such as tingling, burning, pins and needles, numbness and weakness in the affected arm.
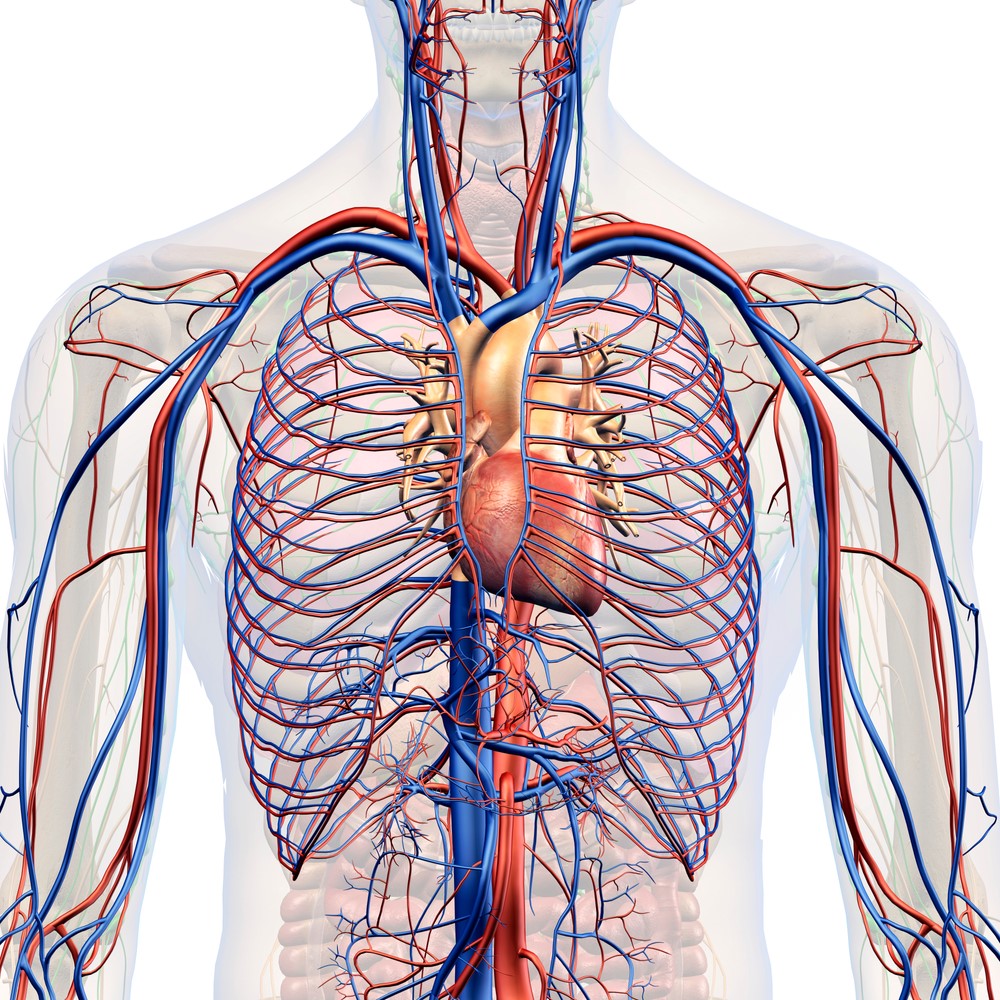
Blood Vessel Injury
Major blood vessles running closly to the shoulder joint can become obstructed. This can give rise to similar symptoms as above but also colour changes in the hand.
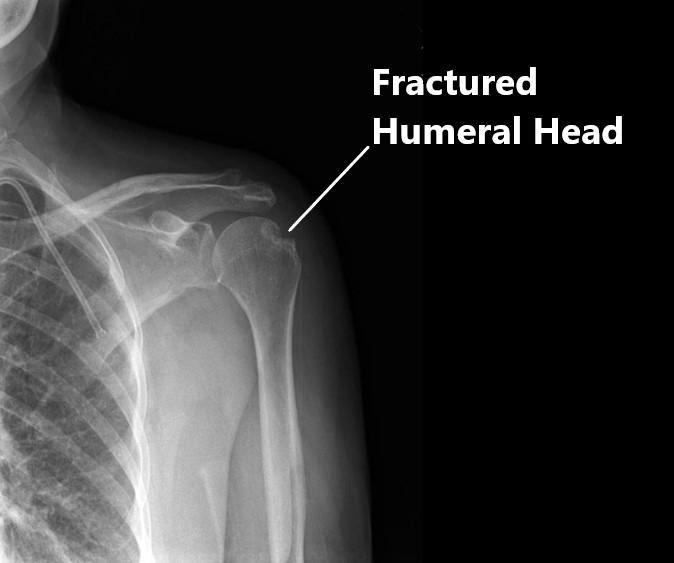
Fractures
Impact of the bony joint surfaces following a dislocation can result in small fractures to the ball against the socket. These injuries generally require surgery.
Joint Cartilage Injuries
Damage to the joint cartilage can also arise from the same mechanism as described above. This will predispose you to an early onset of arthritis.
Labral Tear
The labrum can be scuffed off the socket as the ball is displaced out of the joint. These injuries generally require surgery.
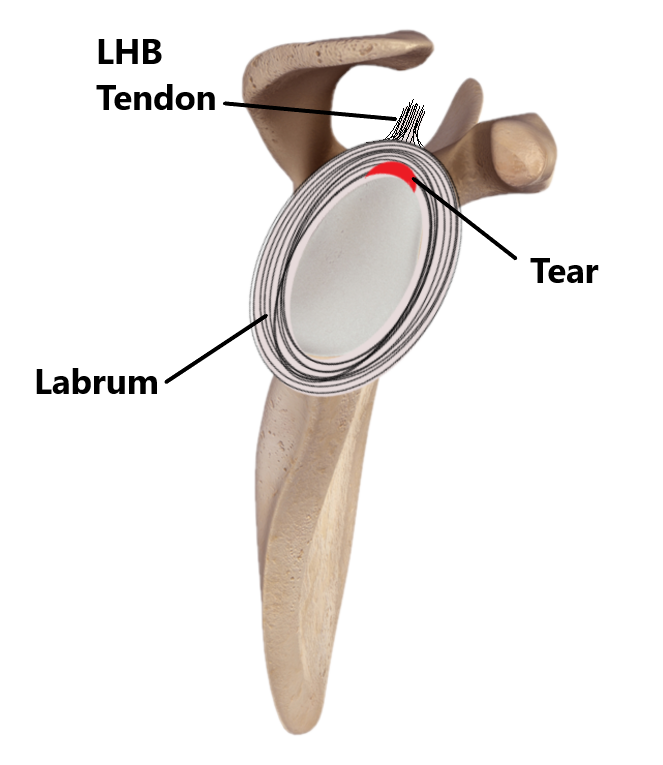
Labral Tear (Bankart Lesion) Following Anterior Shoulder Dislocation
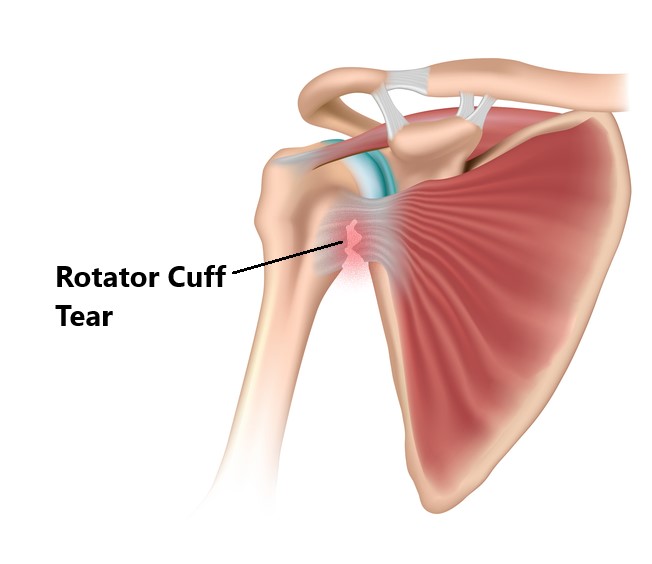
Rotator Cuff Tears
Following a dislocation, tears to the rotator cuff are most commonly seen in people from middle age and on wards. 80% of people >60 years will sustain a cuff tear following a dislocation. Traumatic cuff tears generally require surgery.
Common Symptoms of Subluxations and Shoulder Dislocations
Subluxation
- heaviness and dragging
- “dead arm” feeling especially after activity
- instability and apprehension to move shoulder in certain positions
- lack of power
- pins and needles and numbness in arm

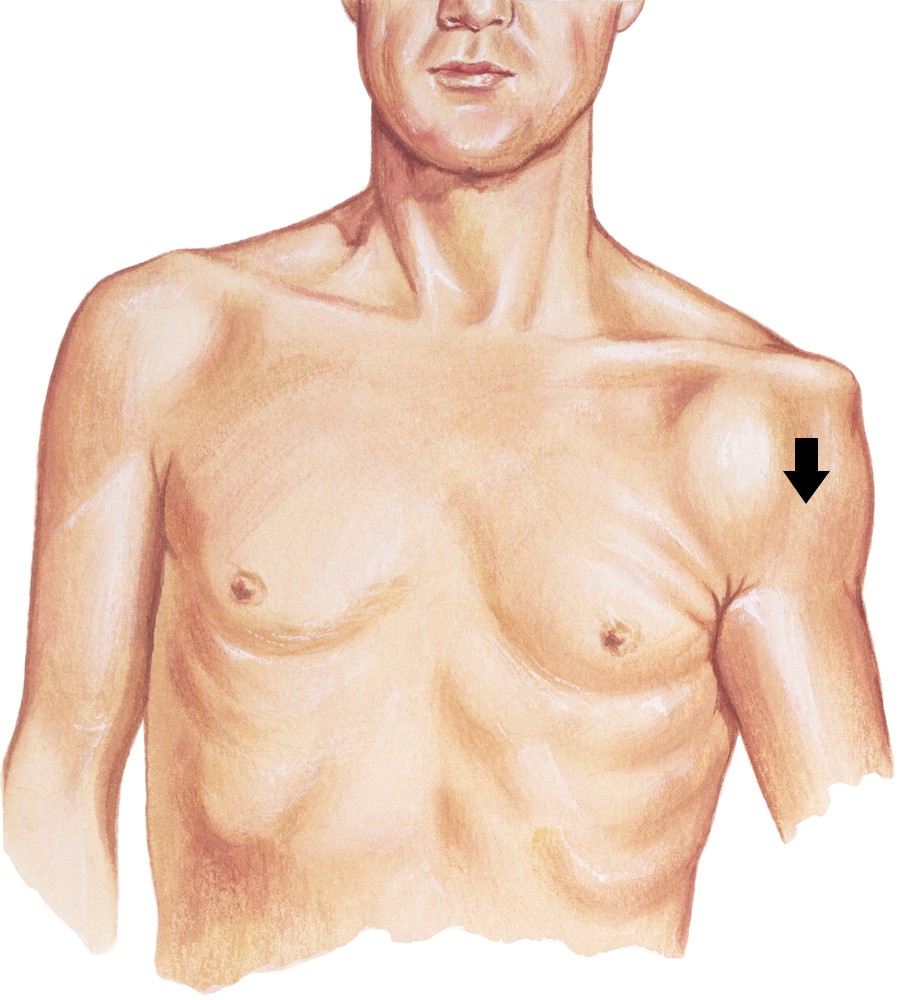
Dislocation
- joint deformity
- intense pain
- inability to use arm
- pins and needles and numbness in arm

Note: drooping position of shoulder
Shoulder Dislocation Risk Factors
- participating in over head sports
- participating in contact sports
- history of subluxations/dislocations
- joint hypermobility
- young (<25 years of age) active males

Management of Shoulder Dislocations
- First and foremost, following an acute shoulder dislocation our priority is to relocate the joint to minimise the risk of nerve/blood vessel damage. If this does not happen spontaneously please seek urgent medical attention, more damage can be inflicted if not done correctly (i.e. nerve and blood vessel damage, fractures) in a timely manner.
- After the joint has been relocated an x-ray should be preformed to screen for potential fractures, a physical examination should be performed by a trained health professional to assess for secondary nerve/blood vessel damage.
- Once cleared, a shoulder sling should be worn for 3-6 weeks. Excessive stretching movements of the arm should also be avoided to enable the ligaments to heal.
- Commencement of conservative physiotherapy treatment is generally recommended as a first line of treatment.
- In cases of recurrent dislocations (despite physiotherapy treatment), surgery may be required to increase the stability between the ball and socket by tightening the joint capsule or grafting bone onto the socket.

Physiotherapy Management
- Following an acute injury our priority is to minimise the extent of damage, reduce inflammation and decrease pain. Modalities such as RICE (Rest, Ice, Compression, Elevation), strapping, manual therapy and acupuncture may also be used.
- Provide education, address unhelpful beliefs regarding the injury, identify and modify aggravating factors
- Continually to reassess the shoulder for secondary injuries.
- Restore pain free shoulder and elbow range of motion and prevent secondary complications (i.e. development of a frozen shoulder). Commence movement and stretching exercises.
- Strengthen the rotator cuff and muscles surrounding the shoulder blades. Commence a graded strengthening program.
- Identify and address movement and postural issues that may have contributed to the injury (i.e. stooped posture, poor positioning of the shoulder blades, lack of spine/hip mobility).
- Graded return to work, sport and function.

Please keep in mind the information provided is general in nature and should not be used as a substitute to consult your treating health professional. If you have any specific questions or require assistance with your individual treatment requirements please do not hesitate to contact My Family Physio in Pittwater Place Shopping Centre in Mona Vale.
Related Articles