Articles Shoulder Impingement
Shoulder impingement refers to pain experienced in the shoulder as the arm is raised towards 90 degrees. This is one of the most commonly reported symptoms of people who have shoulder pain.
Basic Anatomy
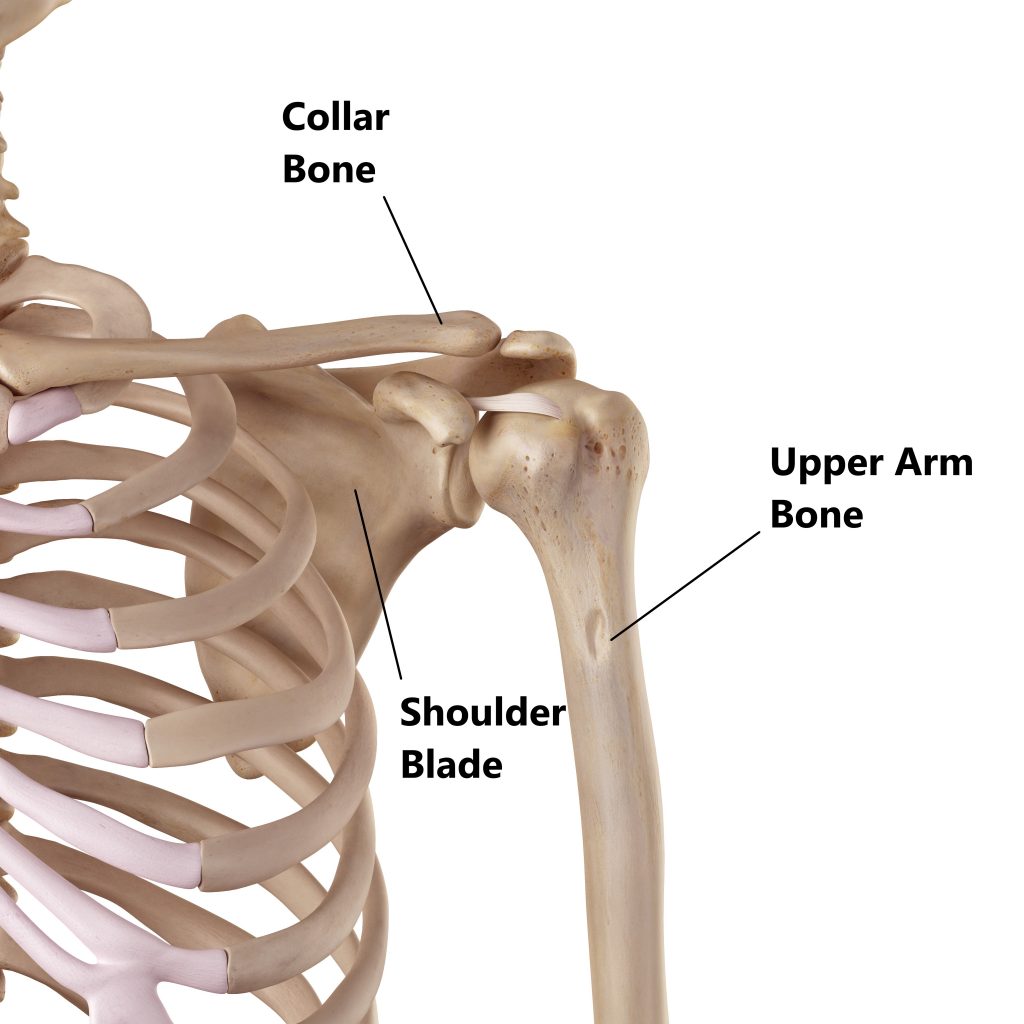
The shoulder joint is comprised of 3 bones:
- collar bone (clavicle)
- upper arm bone (humerus)
- shoulder blade (scapula)
A ball and socket joint is formed between the humerus and scapula. Above this, the collar bone connects to a different part of the scapula called the acromion.
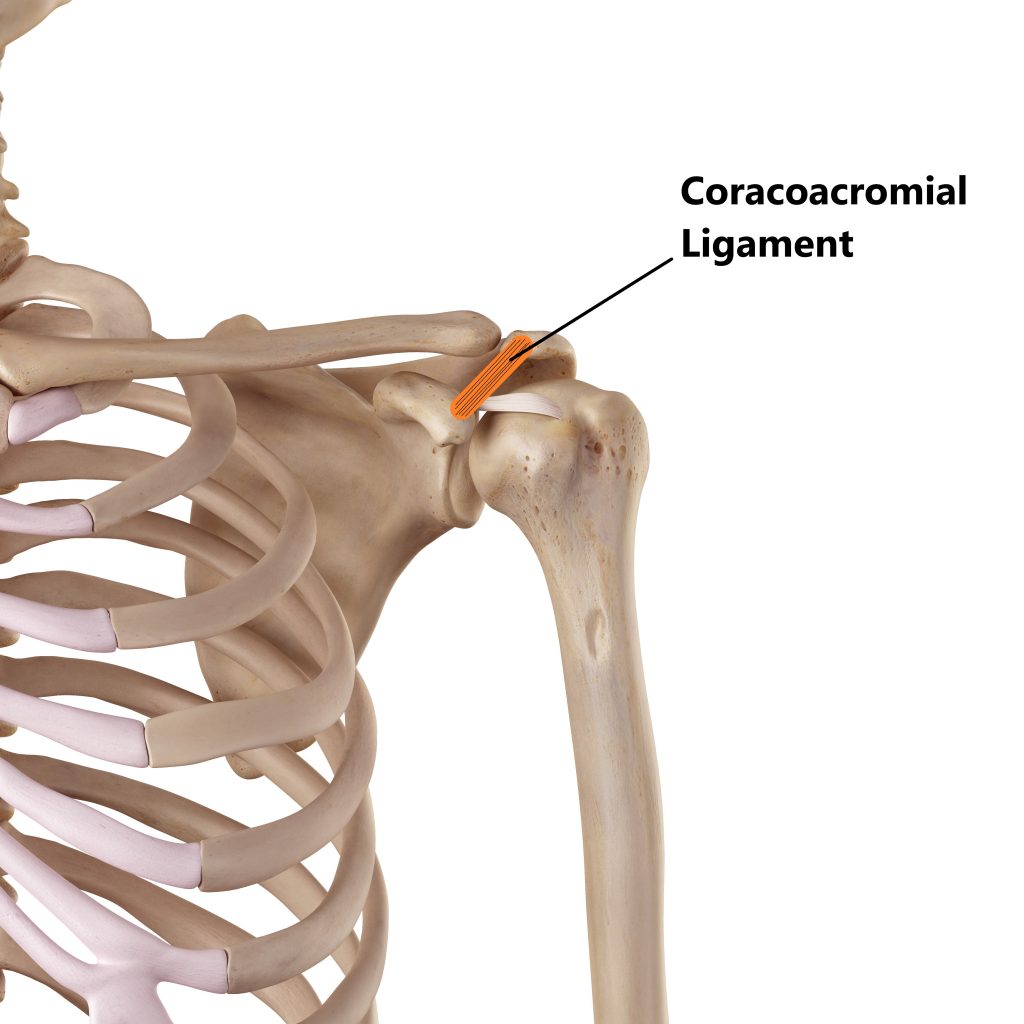
To help provide more stability, a ligament (coracoacromial ligament) is formed between the 2 bony processes (acromion and corocoid process) of the scapula.
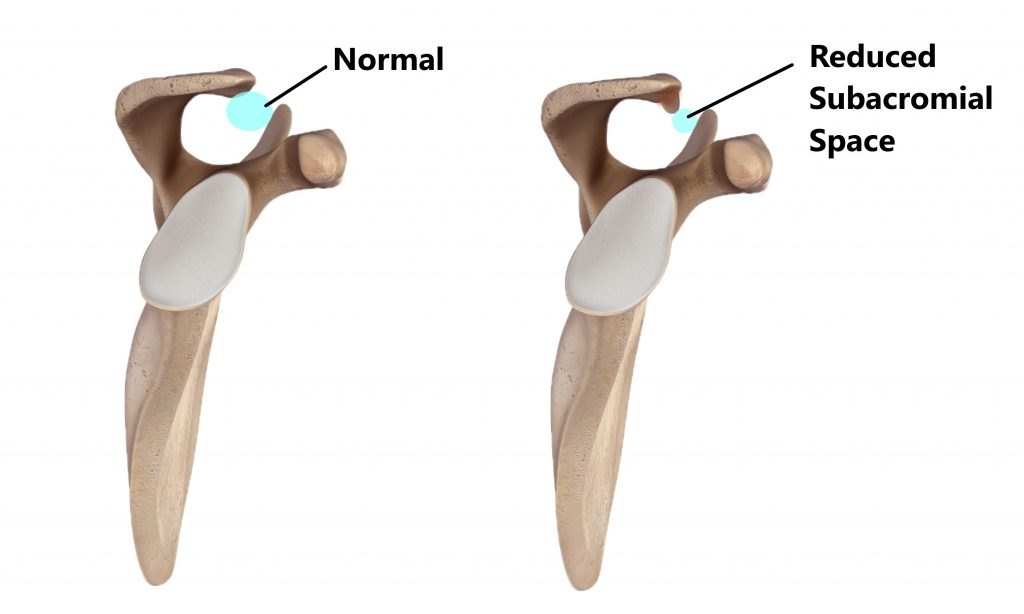
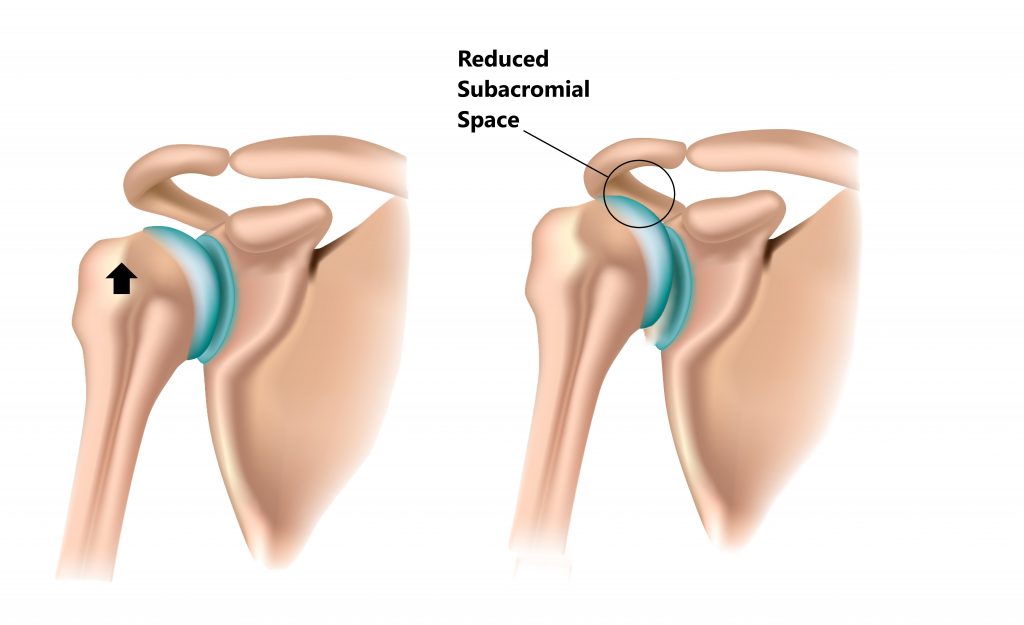
The area between this ligament and the head of the upper arm bone is known as the “subacromial space”.
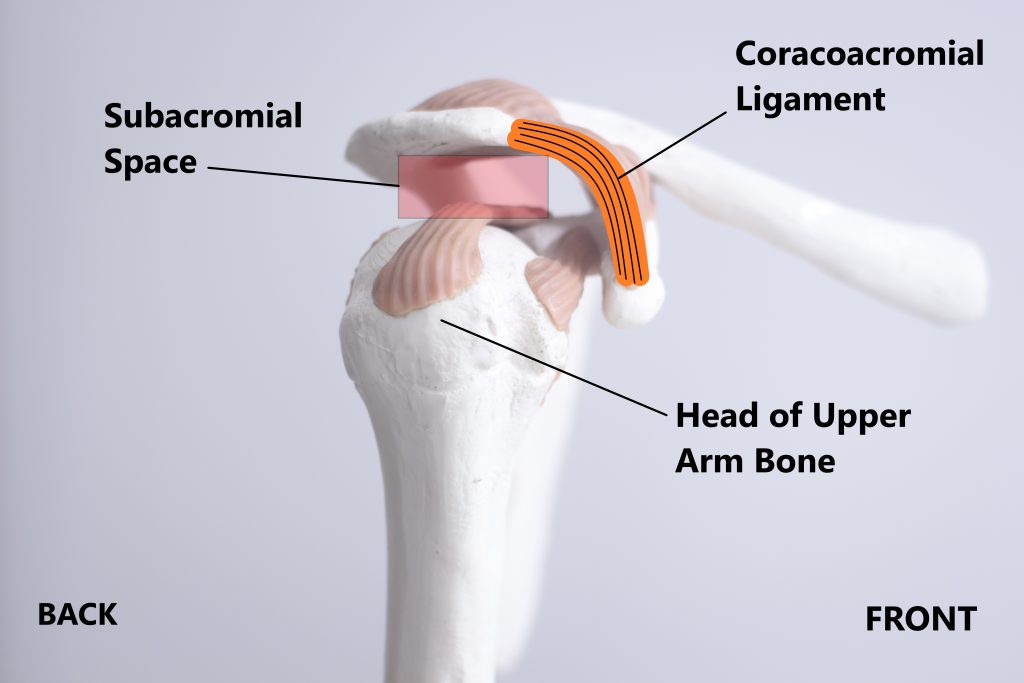
Anatomically speaking this is a very busy area in that we have a few structures occupying a small space:
- longhead of the biceps tendon
- supraspinatus tendon (one of the tendons of the the rotator cuff)
- a fluid filled sack called the subacromial bursa
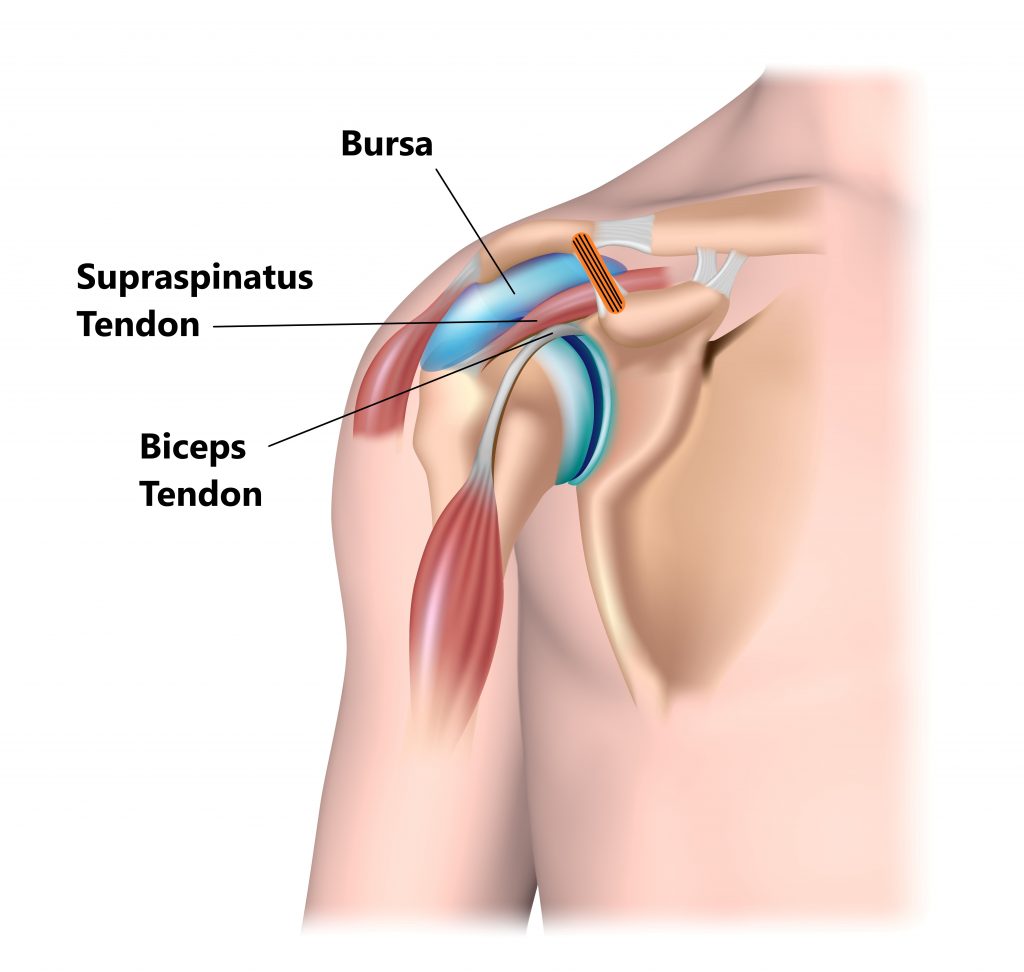
A reduction in size of the subacromial space can lead to these structures being squished between the ligament and the head of the upper arm bone when elevating the shoulder towards 90°. This is known as subacromial impingement.

Causes of Shoulder Impingement
Shoulder impingement can be due to multiple causes. All the below injuries reduce the size of the subacromial space and can give rise to shoulder impingement.
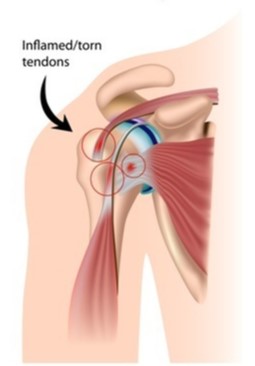
Tendon Injuries
Tendinitis and tendon tears of the supraspinatus and long head of biceps tendons can give rise to inflammation and swelling.
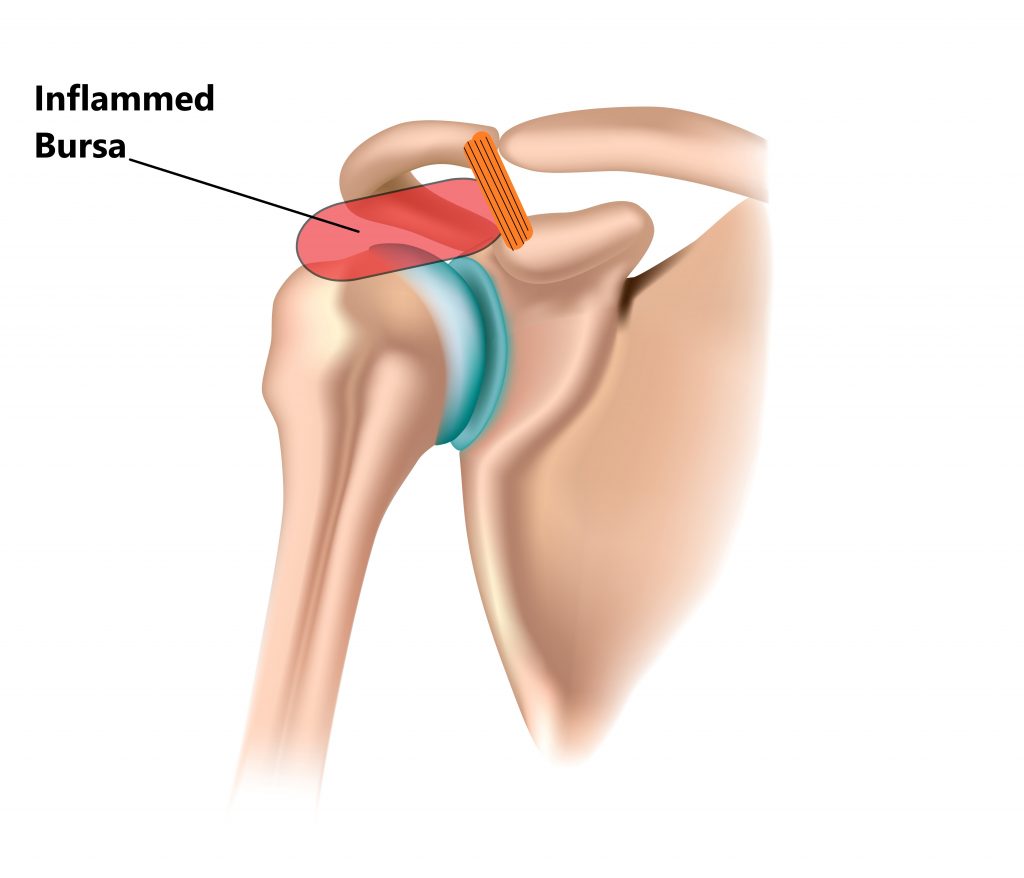
Subacromial Bursitis
Inflammation of the subacromial bursa can give rise to swelling and compression.
Abnormally Shaped Acromion
In some individuals the end of the acromion will grow in a downwards direction and reduce the subacromial space. If symptomatic, these problems may require surgical intervention.
Bone Spurs/Osteophytes
Chronic shoulder injuries, trauma and surgery can give rise to small outgrowths of bone forming on the under side of the acromion. This is more commonly seen in older individuals and may require surgery.
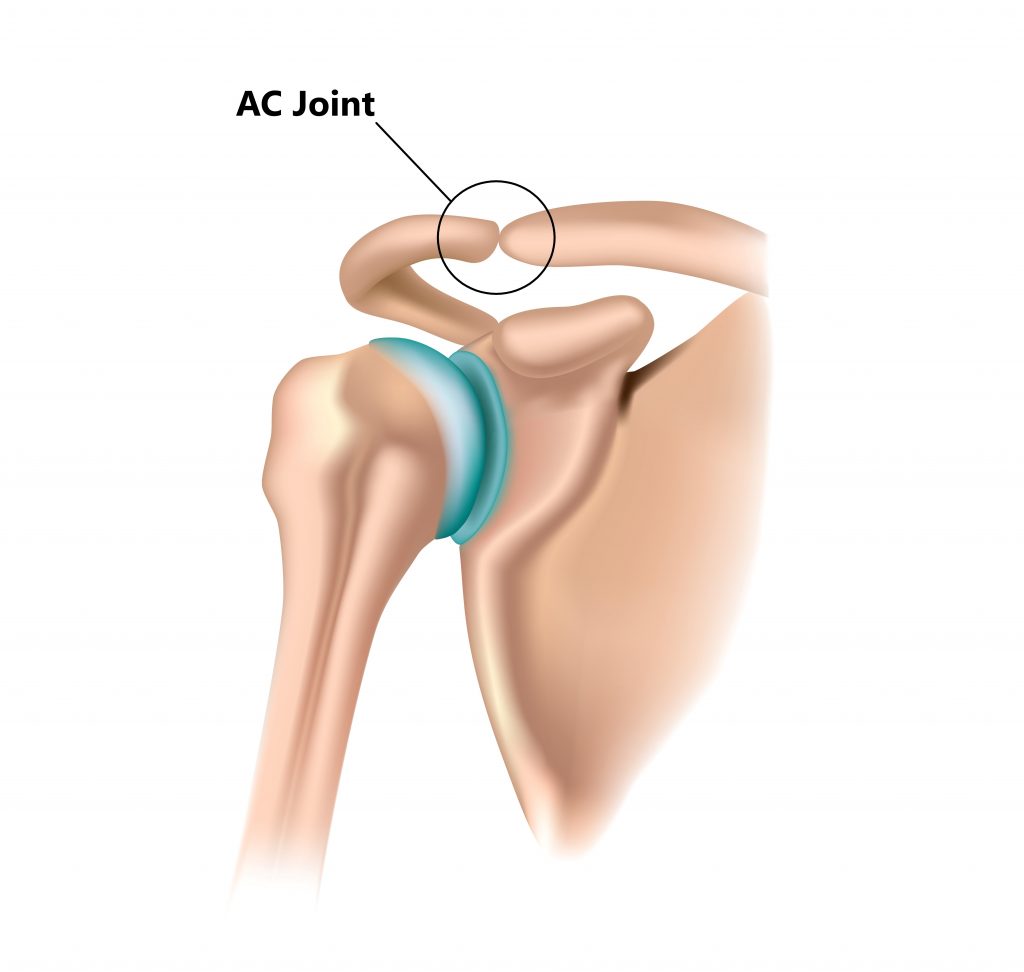
Acromioclavicular joint (AC joint) Injuries
The AC joint is located above the subacromial space. Damage to the joint and can lead to inflammation and thickening of the bone which can reduce the subacromial space.
Shoulder Instability
Loose ligaments (i.e. following a shoulder dislocation) or a weak rotator cuff can lead to a lack of stability between the ball and socket joint of the shoulder. This makes it easier for the ball to shift in an upwards direction thereby reducing the subacromial space.
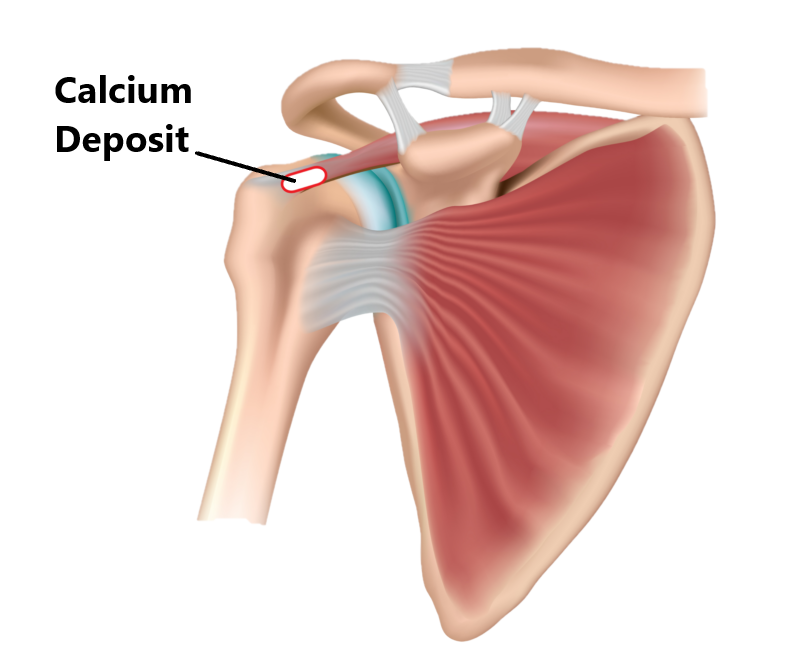
Calcificaion
Calcium deposits can form within tendons and ligaments, this is more commonly seen in older individuals and those with chronic shoulder injuries
Poor Posture
Poor posture and muscle imbalances can lead to impingement. To appreciate this firstly stand tall and raise your arms above your head. Now, let yourself slump and raise your arms again. You may notice how much more uncomfortable it is to raise your arms when in a slumped position.

Internal Shoulder Impingement
Internal shoulder impingement is a lot less commonly seen amongst the general population. This condition is normally observed in people who engage in overhead throwing sports such as baseball.
During the wind up phase of the throwing motion the ball pivots on the socket, as the arm accelerates a lot of forces are placed through the shoulder joint. This repeated action can result in specific muscles of the rotator cuff being squished up against the socket of the shoulder.
Correction of muscle imbalances and correction of technique are an integral part of treating this condition successfully.

Symptoms
- Significant increase in pain as the arm is elevated towards 90 degrees
- pain with over head activities
- pain running down the side of the arm
- pain reacing out for objects
- painful click as arm is raised away from body
Risk Factors
- Engaging in occupations involving repeated overhead activity
- Engaging in sporting and recreational activities involving repeated overhead activity
- Previous trauma (i.e. fractures , dislocations, previous surgery)

Diagnosis
As demonstrated above shoulder impingement can be due to multiple factors. In order to prevent recurrances it is important to have an accurate diagnosis and treat the root cause. Diagnosing shoulder impingement is based on an individuals clinical examination and imaging. In many cases imaging is not always necessary.
- Subjective examination
- Physical examination
- Xray
- Ultrasound
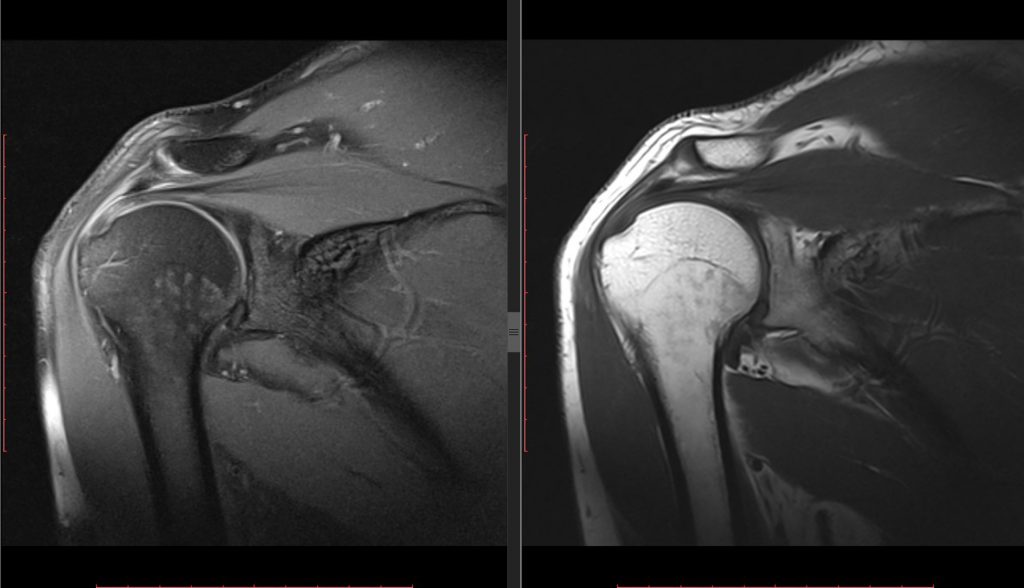
- MRI
Management
Most cases of shoulder impingement will resolve with conservative physiotherapy treatment (see below). Non conservative treatment such as cortisone injections and surgery may be considered if symptoms continue to persist and physiotherapy treatment is unsuccessful.

Physiotherapy Management
Shoulder impingement is typically managed with conservative physiotherapy treatment.
- Following an acute injury our priority is to minimise the extent of damage, reduce inflammation and decrease pain. Modalities such as RICE (Rest, Ice, Compression, Elevation), strapping, manual therapy and acupuncture may be used.
- Provide education, address unhelpful beliefs regarding the injury, identify and modify aggravating factors
- Restore pain free shoulder range of motion and prevent secondary complications (i.e. development of a frozen shoulder). Commence movement and stretching exercises.
- Strengthen the rotator cuff and muscles surrounding the shoulder blades. Commence a graded strengthening program.
- Identify and address movement and postural issues that may have contributed to the injury (i.e. stooped posture, poor positioning of the shoulder blades, lack of spine/hip mobility).
- Graded return to work, sport and function.

Please keep in mind the information provided is general in nature and should not be used as a substitute to consult your treating health professional. If you have any specific questions or require assistance with your individual treatment requirements please do not hesitate to contact My Family Physio, Northern Beaches Sydney.
Related Articles