Articles Rotator Cuff Injuries
This article outlines simple anatomy, common injuries and management principles to give you a good basic understanding of the rotator cuff.
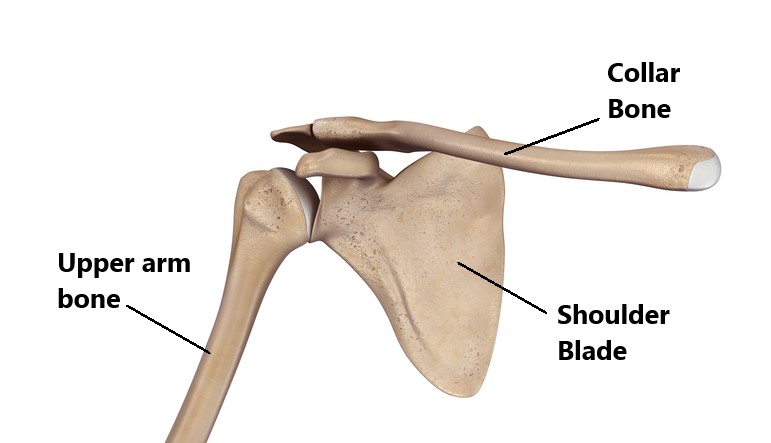
Basic Anatomy
The shoulder joint is a shallow ball and socket much like a golf ball sitting on a tee. Nature has designed our shoulders for movement therefore our bodies rely heavily on the surrounding muscles, tendons and ligaments to provide stability.
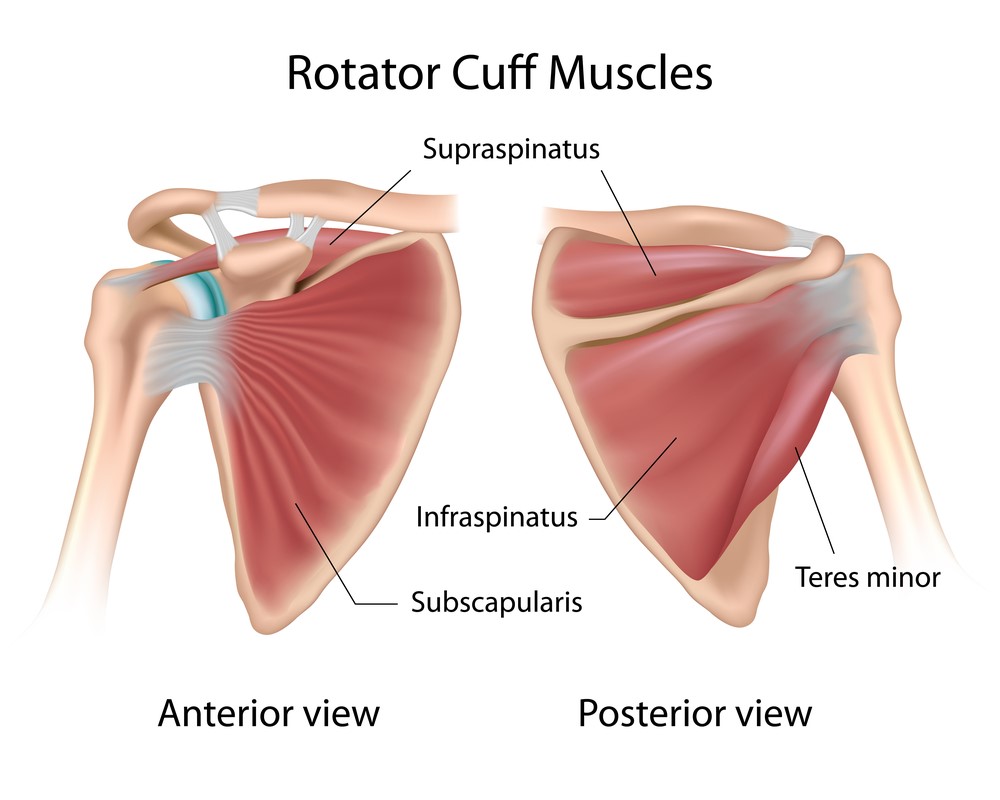
What is the Rotator Cuff?
The rotator cuff is a group of 4 muscles:
- Supraspinatus
- Subscapularis
- Infraspinatus
- Teres minor
They arise from the shoulder blade and their tendons all attach onto the “ball” of the shoulder. Their primary role is to keep the “ball” centred on the “tee” while the shoulder moves through range.
Injuries to the Rotator Cuff
Some common rotator cuff injuries have been listed below. Of the 4 tendons the supraspinauts and subscapularis are the most often injured.
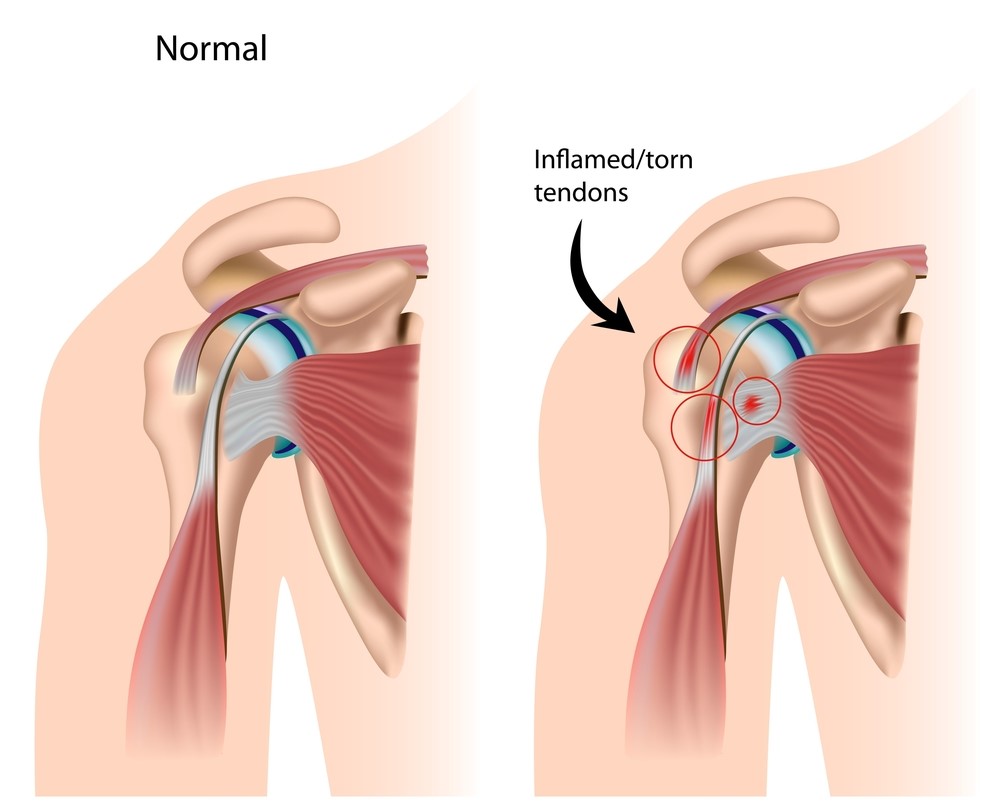
Tendinitis
The tendons of the rotator cuff can become inflamed and painful following an acute trauma (i.e. fall, lifting a heavy object in an awkward position) or from overuse (i.e. repeated over head actives such as swimming, tennis, painting a ceiling). These injuries are typically managed conservatively. Occasionally a cortisone injection may be required to alleviate inflamation.
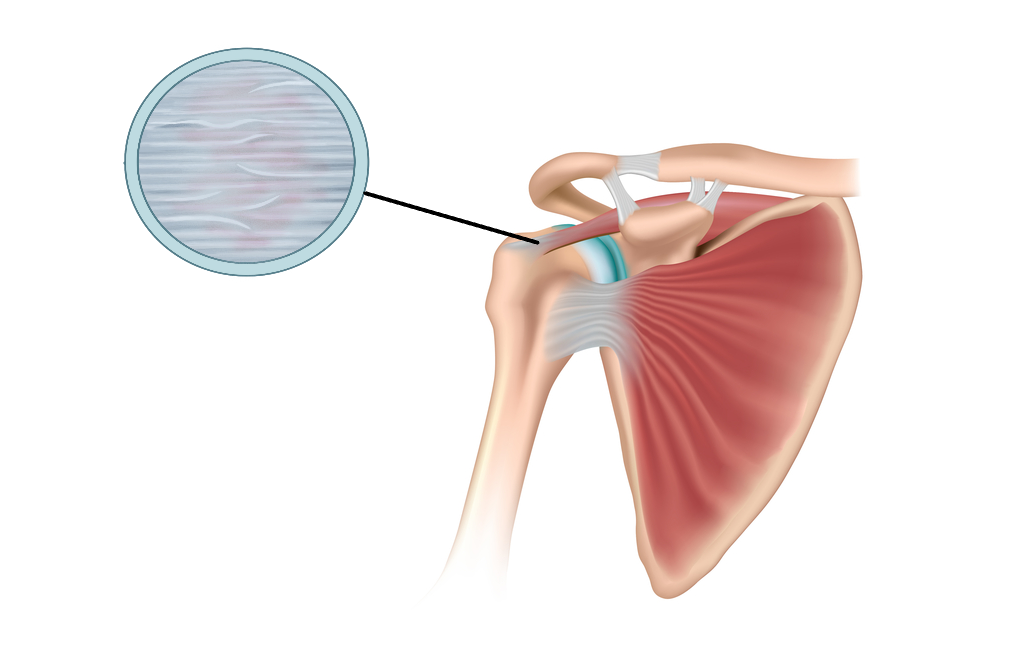
Tendinosis
This is most commonly seen in people from middle age and on wards, it is the result of overuse and natural wear and tear. Tendinosis is
characterised by thinning and weakening of the tendon making you more prone to developing tears. This condition lacks of the presence of inflammation therefore, does not respond well to anti-inflammatory medications. These injuries are best managed conservatively.
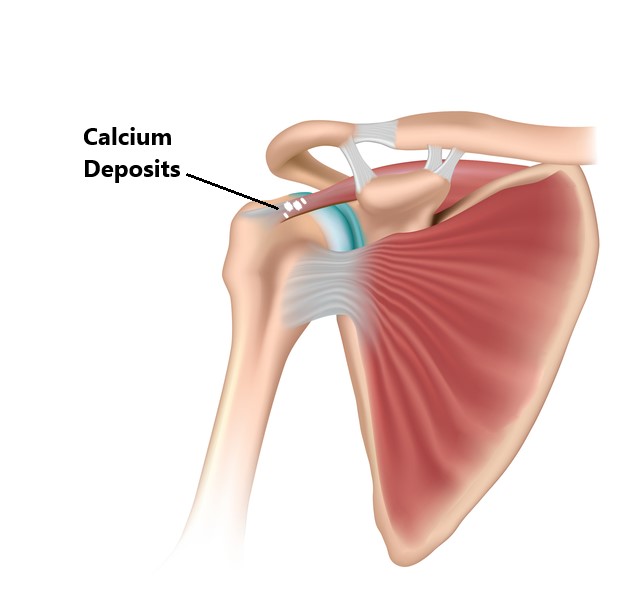
Calcific Tendinitis
This condition is characterised by calcium deposits forming inside the tendons. It is unclear why this occurs but is more often seen in diabetics and in people from middle age and on wards. In most cases the body will reabsorb the calcium deposits. Occasionally non conservative procedures are required to reduce/remove the deposits such as needle aspiration, ultrasound therapy, arthroscopic surgical removal.
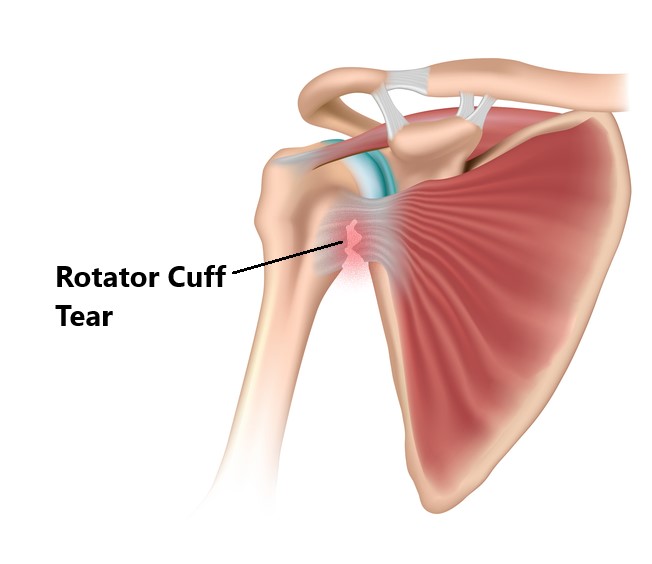
Tendon Tears
Rotator cuff tears range from partial tears to complete ruptures and can be classified into 2 categories:
Acute Tears, are generally the result of acute sudden trauma such as a fall. Small to moderate sized tears are best managed with conservative treatment, occasionally a cortisone injection may be required to alleviate inflammation. Larger tears may require surgical repair.
Degenerative Tears, are more common amongst the general population and a normal part of the ageing process. These are generally due to wear and tear and overuse (i.e. overhead sports/occupations). As we age the blood supply to our tendons lessen making it easier to develop tears. Studies have found up to 50% of people above the ages of 60 with no shoulder symptoms will have a cuff tear. Degenerative tears do not necessarily require treatment unless the individual is symptomatic. Treatment typically consists of conservative physiotherapy management.
Risk Factors for Rotator Cuff Injuries
- People who are < 40 years of age
- People who engage in occupations and sports involving repeated and prolonged over head activity (i.e. Painters, Volley ball players)
- History of previous shoulder trauma (i.e dislocation, fracture)
- Diabetics

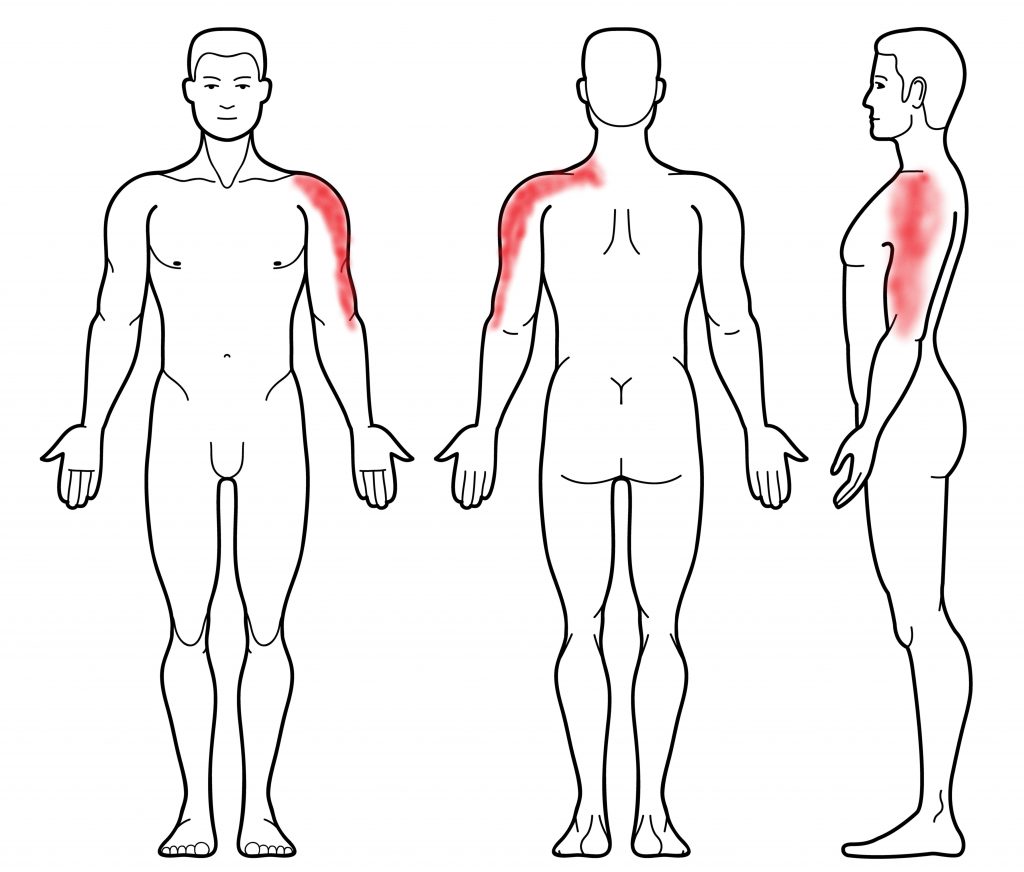
Symptoms of A Rotator Cuff Injury
- weakness
- difficulty lifting the arm for over head tasks (i.e . washing hair)
- deep ache in the shoulder, can have pain running down the side of the arm
- pain when elevating the arm to shoulder height (impingement)
Other Associated Injuries
More often than not rotator cuff injuries do not occur in isolation. Other commonly associated injuries include:
- subacromial impingement
- shoulder bursitis
- injury to the long head of biceps tendon
- Osteoarthritis of the glenohumeral joint
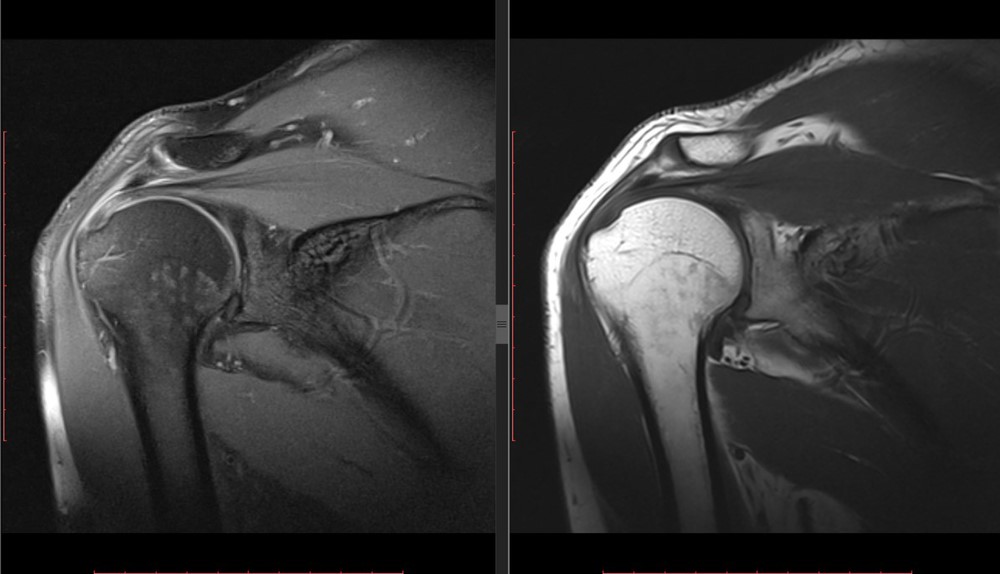
Diagnosis
Diagnosing a rotator cuff injury is based on an individuals clinical presentation and imaging. In many cases imaging is not always necessary.
- Subjective and Physical Examination
- Xray
- Ultrasound
- MRI
Physiotherapy Management
- Following an acute injury our priority is to minimise the extent of damage, reduce inflammation and decrease pain. Modalities such as RICE (Rest, Ice, Compression, Elevation), strapping, manual therapy and acupuncture may be used.
- Provide education, address unhelpful beliefs regarding the injury, identify and modify aggravating factors
- Restore pain free shoulder range of motion and prevent secondary complications (i.e. development of a frozen shoulder). Commence movement and stretching exercises.
- Strengthen the rotator cuff and muscles surrounding the shoulder blades. Commence a graded strengthening program.
- Identify and address movement and postural issues that may have contributed to the injury (i.e. stooped posture, poor positioning of the shoulder blades, lack of spine/hip mobility).
- Graded return to work, sport and function.

Please keep in mind the information provided is general in nature and should not be used as a substitute to consult your treating health professional. If you have any specific questions or require assistance with your individual treatment requirements please do not hesitate to contact My Family Physio Mona Vale, Sydney.
Related Articles