Articles Musculoskeletal Injuries in Children and Teenagers
Children and teenagers commonly present to physiotherapy clinics. Their bodies are still growing making them more prone to certain injuries when compared to adult populations. It is important to accurately diagnose and identify the cause of these injuries as this will direct treatment to ensure the best outcome.
Tendon Attachment Sites (Growth Plate Traction Injuries)
The growth plates are located towards the ends of bones (see below) and where a tendon inserts onto the bone. The tendon attachment sites in children are relatively weak and more prone to injury, they are less likely to strain a muscle or tendon. Interestingly, the equivalent injuries in adults would present as tendinitis (i.e. Achilles and patella tendinitis).
Common sites include:
- back of the heel (Sever’s disease)
- directly underneath the knee cap ( Sinding-Larsen-Johansson disease)
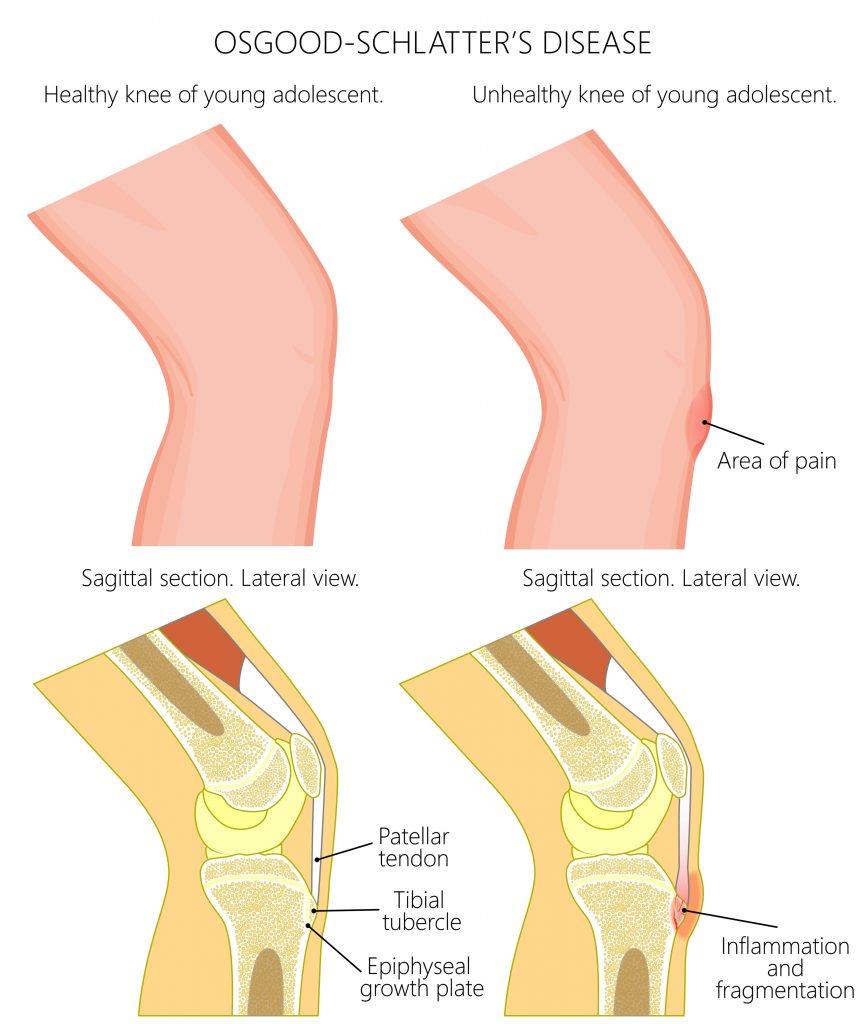
- below the patella tendon (Osgood-Schlatter’s disease)
This is typically an over use condition and commonly seen in highly active children and teenagers. Symptoms include pain during and after activity, swelling, tenderness and thickening of the bone (in Osgood-Schlatter’s disease) at the attachment site. Moderation of activity is an integral part of the managing this condition.
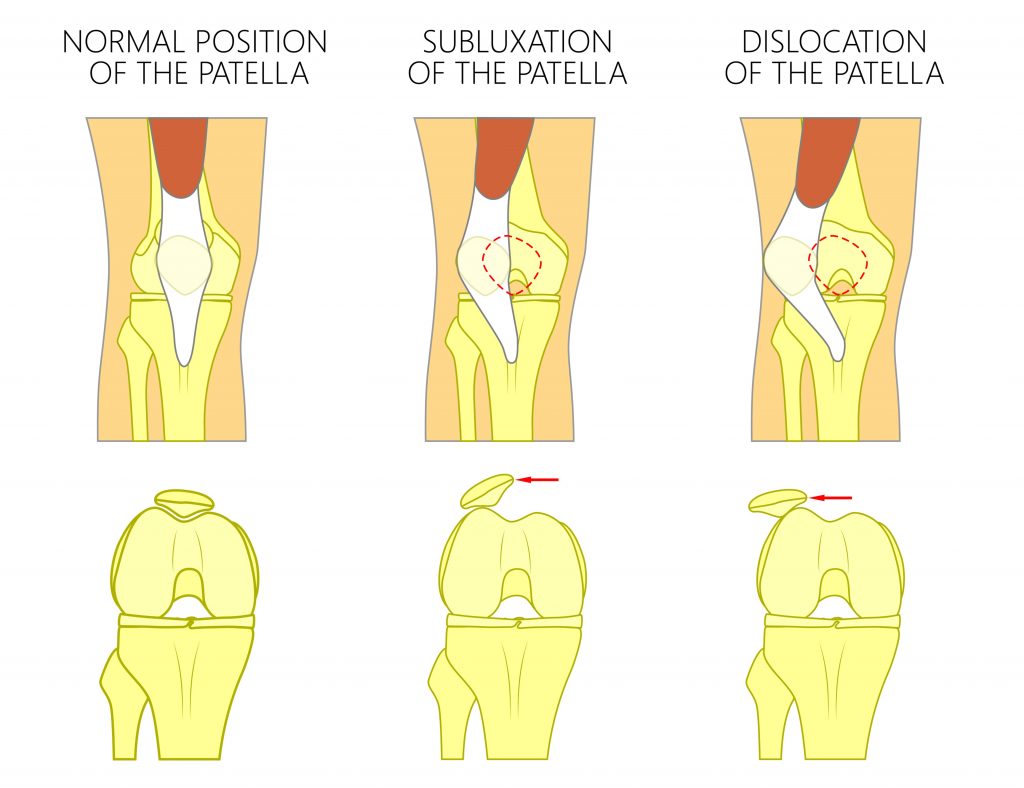
Patella Dislocations and Subluxations (Partial Dislocation)
This occurs when the knee cap is completely (dislocated) or partially (subluxed) displaced out of its normal position. These typically occur following a traumatic incident where an individual suddenly pivots on one leg (i.e. changing direction when sprinting) or following a hard blow to the knee (i.e. tackle).
In the majority of cases the kneecap is displaced laterally away from the mid line. These are most commonly seen in athletic female teenagers. Symptoms can include joint deformity, instability, sudden severe pain and swelling and difficulty weight bearing.
Risk factors include:
- generalised joint hypermobility
- high riding kneecaps (patella alta)
- family history
- abnormal standing postures ( i.e. knock kneed, flat feet, hyper extending knees, being “pigeon toed”, being “duck footed”)
- anatomical abnormalities of joint between the knee cap and thigh bone (shallow lateral femoral groove)
- muscle imbalances at the knee cap (i.e. weak VMO, tight ITB)
Patella displacements firstly need to be relocated. If they do not occur spontaneously please seek medical assistance, more damage can be caused if not done correctly! It is important to follow up with medical imaging as damage to the joint surfaces and ligaments is common following these events.
Unfortunately, the chance of recurrence is high. Appropriate management is typically comprised of adequate rest (bracing may be required) followed by a rehabilitation program to strengthen specific muscles. In some instances surgery will be required especially if an individual experiences recurrent spontaneous dislocations (i.e. rolling over in bed).
Fractures
A child’s skeleton differs to that of an adult in that their bones are still growing and not yet fully developed. This can give rise to specific types of fractures:
- Greenstick Fractures, Children’s bones are a lot more flexible and “rubbery” than adults. Their bones are more likely to bend and crack (much like bending a green branch of a tree) rather than completely breaking. This is more commonly seen in children < 10 years of age and usually occur as a result of a fall. Common sites of injury involve the bones of the forearms and lower legs.
- Growth Plate Fractures, towards each end of a child’s bones are the cartilage growth plates (epiphysis). These areas are where the bone is actively growing thereby making them particularly susceptible to injury. Fractures involving the growth plates are typically seen in teenagers and can be due to trauma (i.e. fall) or overuse (i.e. competitive sports). Common sites of injury include the wrist, elbow, ankle and hip (slipped capital femoral epiphysis see below).

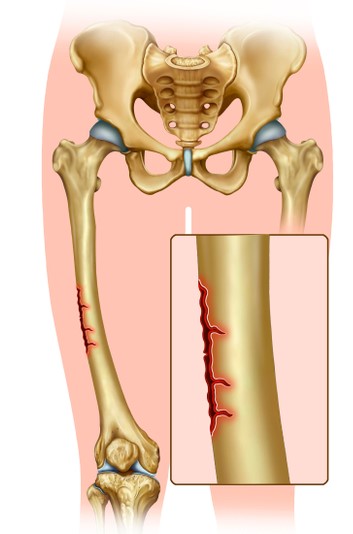
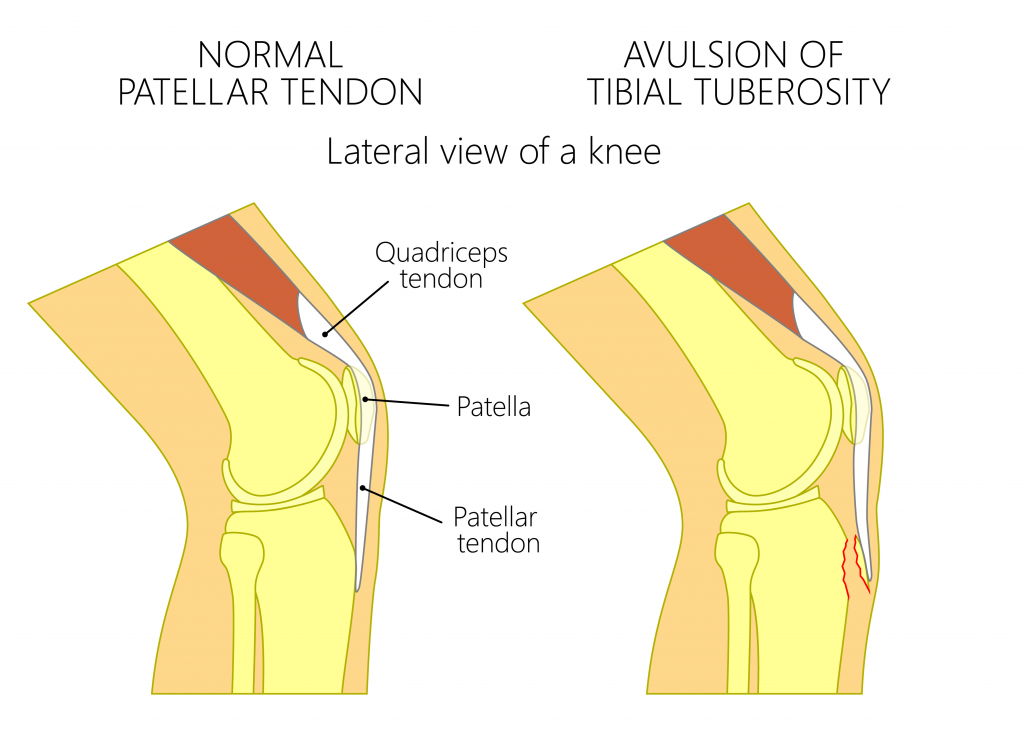
- Avulsion Fractures, in children the tendon attachment sites are relatively weak. They are more likely to partially (as above) or completely pull a tendon off the bone than tear their muscles or tendons. Avulsion fractures arise when a small fragment of bone is pulled off following a forceful muscle contraction (i.e. kicking, jumping, sprinting). These injuries are more commonly seen in teenagers. Common sites of injury include the pelvis, hip and buttock area. Conservative physiotherapy treatment is typically preferred and surgical intervention is rare for this condition.
Symptoms of a fracture can include pain, swelling, joint deformity, bony tenderness and a loss of function. Fractures involving the joint surfaces have more complications and can predispose people to an early onset of arthritis. If you suspect your child has sustained a fracture please seek urgent medical attention, incorrect management can lead to complications and unnecessary ongoing issues.
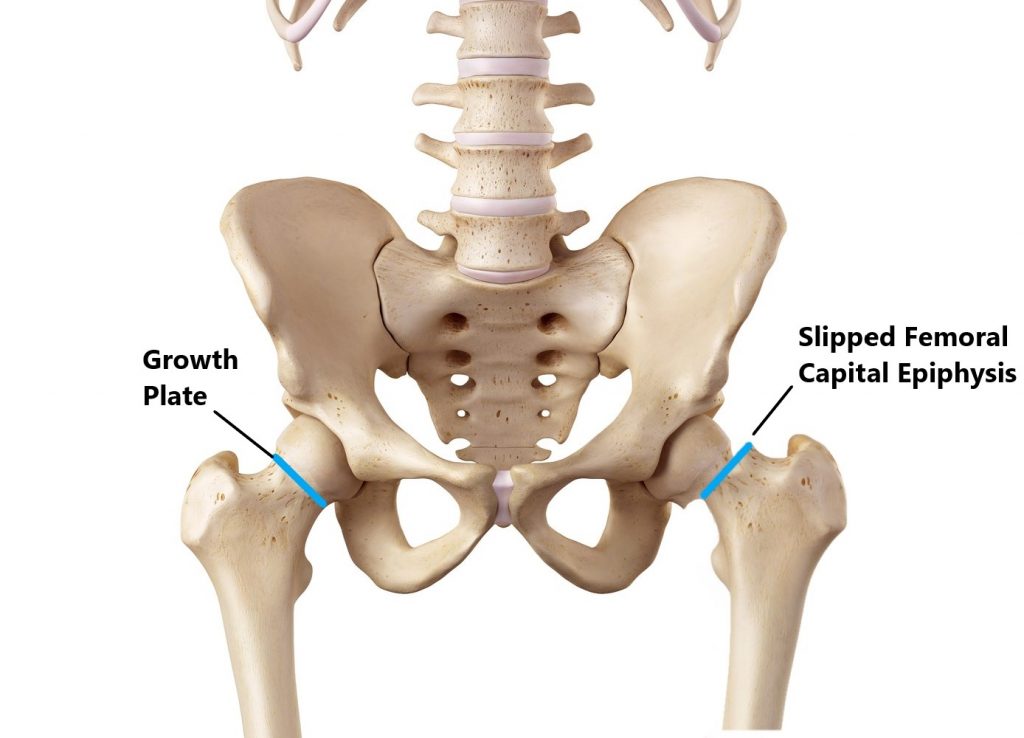
Slipped Capital Femoral Epiphysis
This condition arises due to a fracture through the growth plate of the hip joint resulting in instability. It can occur after trauma (i.e. fall) or gradually over time (more common). The under lying causes are unknown but certain rick factors have been identified:
- obesity
- use of steroid medication
- family history
- metabolic and endocrine disorders
It is most commonly observed in boys between the aged of 11 and 16 years of age and can affect one or both legs. Symptoms can include hip/knee/groin pain, restricted movement, a limp, difficulty/inability with weight bearing, shortening and turning out of the affected leg (becoming duck footed). All suspected cases should be reviewed by an orthopaedic specialist as surgical intervention may be required.
Radial Head Subluxation/Nursemaid Elbow
The ligaments surrounding a child’s elbow are weak making the joint particularly susceptible to partial dislocations. This condition is commonly seen in children between the ages of 1-4 years of age. It typically occurs following an incident where a child’s arm is suddenly pulled. Common mechanisms of injury include:
- swinging a child by the arms
- picking up a child by one arm
- suddenly pulling a child forwards while holding hands
Symptoms can include pain and restricted movement where the child will have difficulty bending the elbow. It is best to seek medical assistance to relocate the radial head to avoid further injury. Please be mindful of this when playing with kids!

Please keep in mind the information provided is general in nature and should not be used as a substitute to consult your treating health professional. If you have any specific questions or require assistance with your individual treatment requirements please do not hesitate to contact MyFamily Physio Mona Vale, Northern Beaches Sydney.