Articles Musculoskeletal Developmental Issues in Children and Teenagers
Children and teenagers commonly present to physiotherapy clinics. Their bodies are still growing making them more prone to certain developmental conditions. It is important to accurately diagnose and identify the cause of these injuries as this will direct treatment to ensure the best outcomes.
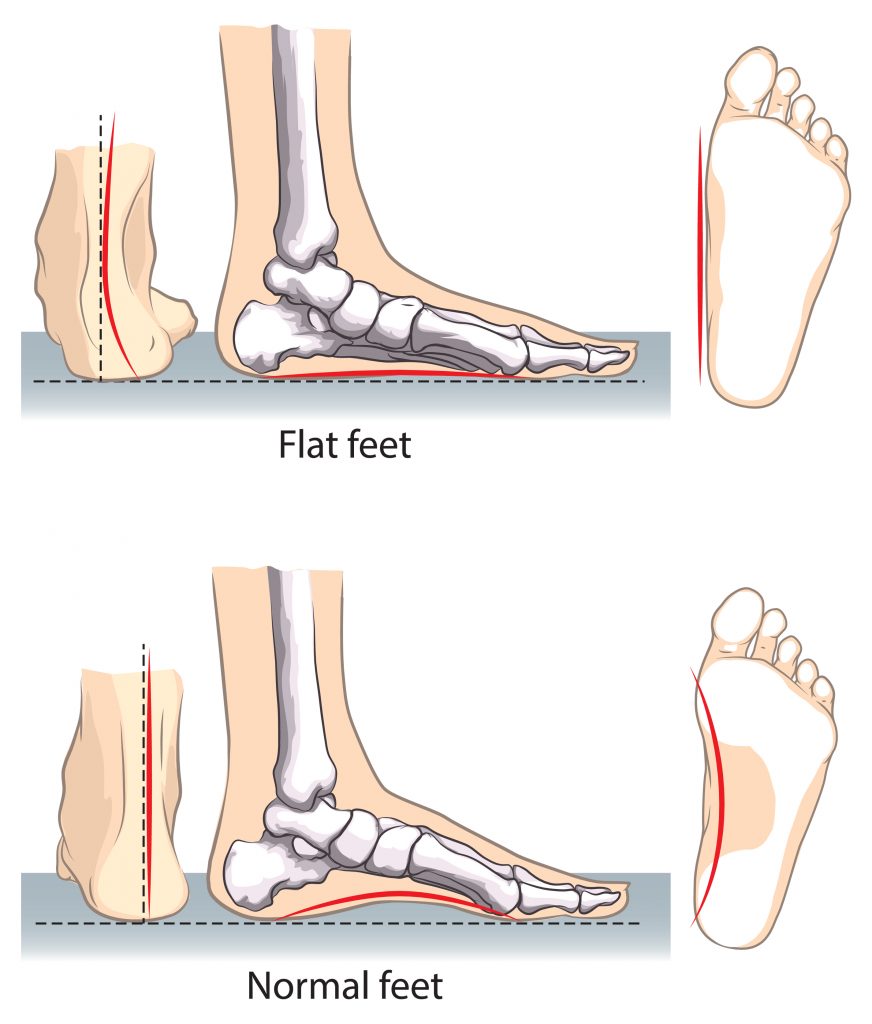
Flat Feet/Pronated Feet/ Pes Planus
Being flat footed is a term used to describe a postural abnormality where the arch on the inner side of the foot is flattened out. In children the arches typically do not develop until 6 yrs of age. A small percentage of individuals will continue to have flat feet into adulthood. This can also gradually develop overtime, being overweight, older age and having diabetes can increase your risk.
Having flat feet places more strain on the muscles, tendons, ligaments and joints which can give rise to a plethora of lower limb (i.e. plantar fasciitis, shin splints, hip impingement) and back problems.
This condition can be separated into 2 categories:
Flexible Flat Feet
- inner arch will be present in non weight bearing positions but not in weight bearing positions.
- do not have to be treated if there are no symptoms
- more common
- typically due to muscle imbalances, tendon tightness (Achilles tendon), overstretched/ruptured tendons/ligaments
- treatment consists of orthotic prescription, stretching and strengthening exercises, casting and bracing
- surgery less common
Rigid Flat Feet
- inner arch with not be present in both weight bearing and non weight bearing positions
- due to structural bony abnormalities in the feet (congenital abnormalities, arthritis)
- presence of foot stiffness (in children)
- should be monitored by a paediatrician (children/teenagers) or an orthopaedic surgeon (if symptoms are severe in adults)
- higher chance of surgery if conservative treatment (as above) is unsuccessful
W Sitting
W sitting is commonly found in children <5 years of age of. It is characterised by sitting on the ground with both hips turning in so that the knees are facing towards each other. Children find this position comfortable because they can rest on their joints and their postural muscles do not have to work very hard to keep them upright. This bad habit can have implications on a child’s development and lead to bigger problems later on in life:
- Lack of core stability, weakness of the trunk muscles limit your ability to sit, stand, run jump and play for prolonged periods of time.
- Poor posture, this can lead to muscle imbalances and movement restrictions resulting in chronic pain.
- Lack of coordination, W sitting makes it difficult to rotate your trunk and use both sides of your body. This can hinder a child’s ability to develop the coordination to use their left and right hands together (i.e. doing up buttons). Similarly, the development of fine motor skills (i.e. writing) can be affected.
- Clumsiness, W sitting encourages your feet to become “pigeon toed” and also makes it difficult to transfer your weight from side to side. This can affect a child’s balance sense making them clumsy on their feet.
- Pain, W sitting places a lot of strain on the hip, knees, spine and feet which can result in chronic pain.
It is always best to correct this bad habit asap before it becomes a major problem later on in life. Some helpful strategies include:
- constantly nagging of your child not to W sit
- encouraging an active lifestyle
- limiting TV, tablet, phone and computer use
- encouraging sitting cross legged, side sitting or long sitting
- encouraging use of both sides of body during play i.e. kicking ball with both feet

Osteochondrosis
This is a group of conditions which affect the growth plates in children and teenagers. It is characterised by an interruption of blood flow and tissue breakdown leading to abnormal bone growth. Unfortunately, the causes of this disease are unknown, it is normally self-limiting and will cease progressing as the bones mature. Symptoms can include restricted movement, pain and swelling over the affected joint/area.
This condition commonly affects the:
- Spine, upper back (Scheuermann’s disease see below)
- Joints, hip joint (Legg-Calve’-Perthes disease see below), foot, wrist and elbow and inside the knee joint (osteochondritis dissecans see below)
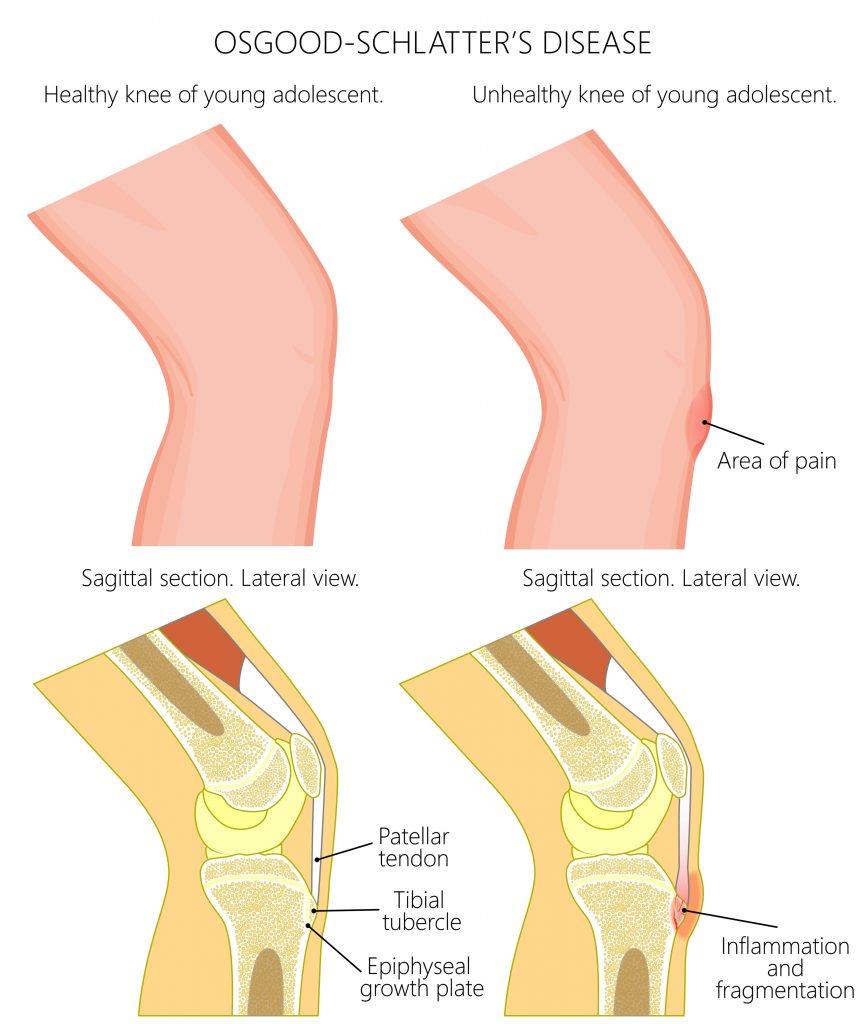
- Tendon attachment sites, back of the heel (Sever’s disease), underneath the knee cap (Osgood-Schlatter’s and Sinding-Larsen-Johansson disease), wrist, elbow and ankle. Interestingly, the equivalent injuries in adults would present as tendinitis (i.e. Achilles and patella tendinitis). The tendon attachment sites in children are relatively weak and more prone to injury, they are less likely to strain a muscle or tendon.
It is important to have these conditions assessed and diagnosed correctly, medical imaging is typically required. Management will vary pending the diagnosis.
Scheuermann’s Disease (Slouching Teenagers)
Scheuermann’s Disease is a developmental condition most commonly observed in teenagers and characterised by abnormal “hunching” of the upper back. This is due to a developmental abnormality where the rear portion of a vertebrae grows faster than the front giving it a “wedged” side profile appearance (much like in OP).
This condition is typically self-limiting and will stop progressing once the spine has reached full maturity. Unfortunately, the causes are unknown. Treatment focuses on pain management, maintaining mobility and strength and limiting the progression of the disease. Only in extremely rare and severe circumstances would surgery be considered (i.e. compromise of heart and lung function).

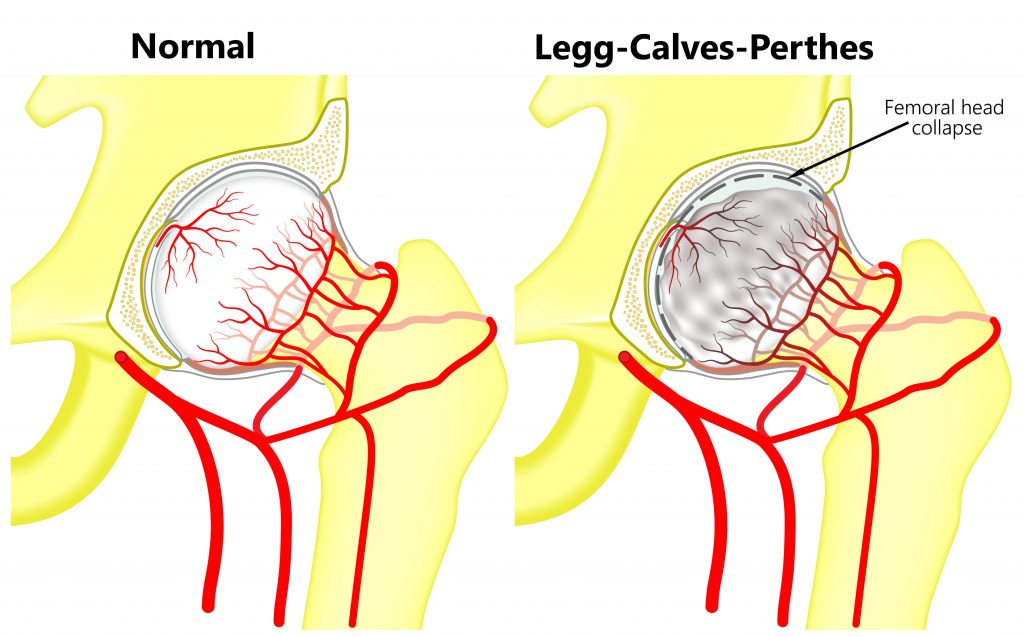
Legg-Calves-Perthes Disease
The hip joint is comprised of a “ball and socket”. In children, a disruption of blood flow to the ball can alter its shape causing the joint to not fit together properly. This rare condition is known as Legg-Calves-Perthes disease unfortunately, the causes are unknown.
It typically affects one leg and is more commonly seen boys between the ages of 4-10 years of age. Symptoms can include hip/knee/groin pain, restricted movement, a limp, difficulty weight bearing and shortening of the affected leg. All suspected cases should be reviewed by an orthopaedic specialist. Most presentations are managed conservatively with physiotherapy treatment. Only in severe circumstances would surgery be considered.
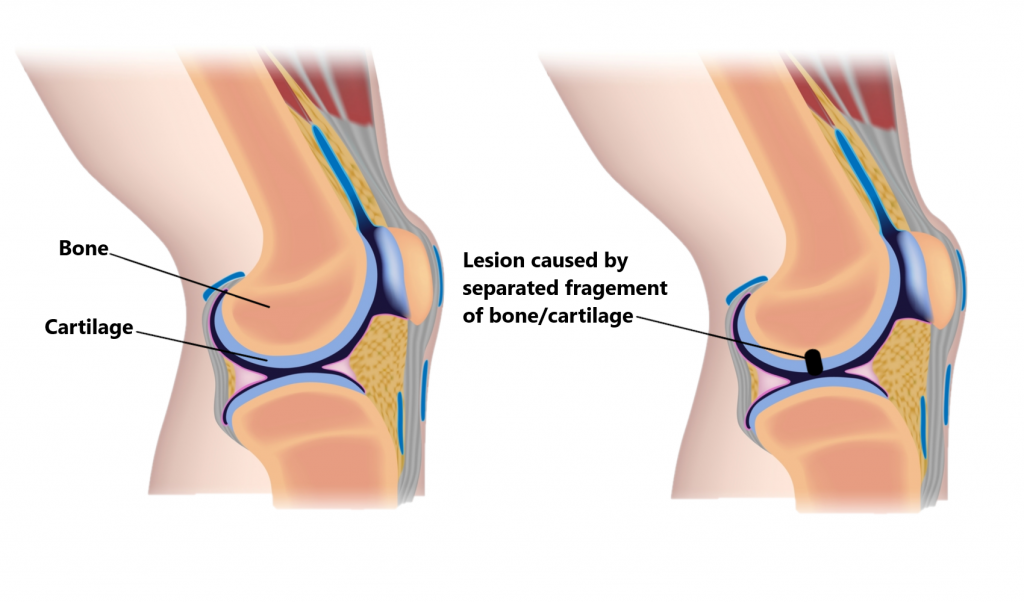
Osteochondritis Dissecans
This condition most commonly affects the knee joint. A disruption of blood flow to the bone underneath the joint cartilage can cause tissue death. Fragments of bone and cartilage can potentially break off causing problems inside the joint. It is typically seen in highly active teenagers. Symptoms can include joint pain/swelling, weakness, restricted movement and joint locking. Moderating activity levels is an important part of management. Occasionally, these injuries can require surgery especially in the presence of joint locking.
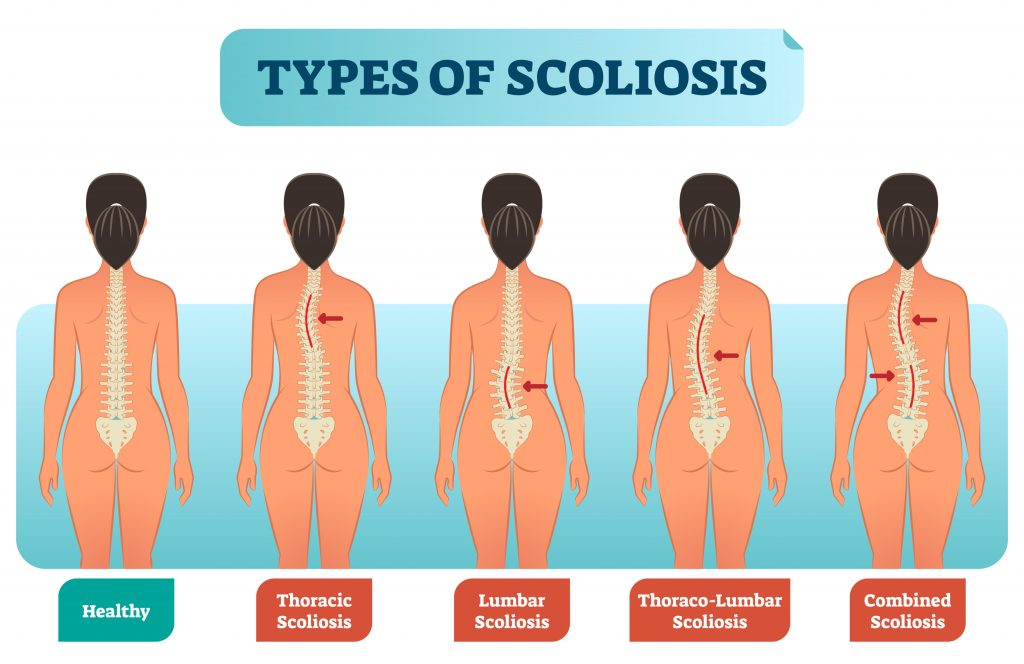
Scoliosis
A scoliosis is an abnormal curvature of the spine. Affected individuals often appear to stand in asymmetrical positions where the shoulders and trunk are not even. There are different types of scoliosis:
- Non-Structural Scoliosis, the deformity of the spine is not fixed, does not progress during development and can be corrected. Muscle imbalances and uneven leg length often contribute to this problem and can be easily modified.
- Structural Scoliosis, the deformity of the spine is fixed and can progress during development.
A Structural Scoliosis can be present from birth or gradually develop during the childhood/teenage years. Causes include:
- anatomical abnormalities of the spine (i.e. abnormal bone growth)
- neuromuscular disorders ( i.e. cerebral palsy)
- weak ligaments/joints/tendons
- diseases of the bone
- unknown causes/Idiopathic Scoliosis
Of these, Idiopathic Scoliosis is the most common typically affecting females between the ages of 10-18 years.
Most cases are mild and will stop progressing as the spine reaches full maturity. X-rays are often required to enable monitoring of the disease. The degree of spinal curvature and age of the individual determines what type of treatment is required. Surgical intervention is rare and only considered in specific situations (i.e. severe spinal curvature, deterioration of spinal alignment, compromise of lung and heart function). Physiotherapy treatment can be beneficial to minimise the impact of this condition.
Growing Pains
Growing pains affect approximately a third of all children particularly between the ages of 3-5 and 8-11 years. It is unclear what the under lying causes are. Generalised muscle pain is typically felt in the legs (i.e. quadriceps, hamstrings and calves). This is more likely to occur towards the end of the day, after activity, before bed and occasionally during the night. Symptoms are not normally present in the mornings. Growing pains are not harmful or causing damage, if your child is experiencing ongoing issues it may be beneficial to have them thoroughly assessed by a health professional to rule out other potential causes. Commencing a program of regular stretches, heat packs, massage and activity modification are often all that is required to manage this condition.

Please keep in mind the information provided is general in nature and should not be used as a substitute to consult your treating health professional. If you have any specific questions or require assistance with your individual treatment requirements please do not hesitate to contact MyFamily Physio Mona Vale, Northern Beaches Sydney.