Articles Cubital Tunnel Syndrome
This article explains basic anatomy, what cubital tunnel syndrome is, causes, risk factors, diagnosis, and physiotherapy management.
Basic Anatomy
The nerves in the upper limbs all arise from the neck. As they descend towards the hands they branch off into 3 main nerves :
- Radial Nerve
- Medial Nerve
- Ulnar Nerve
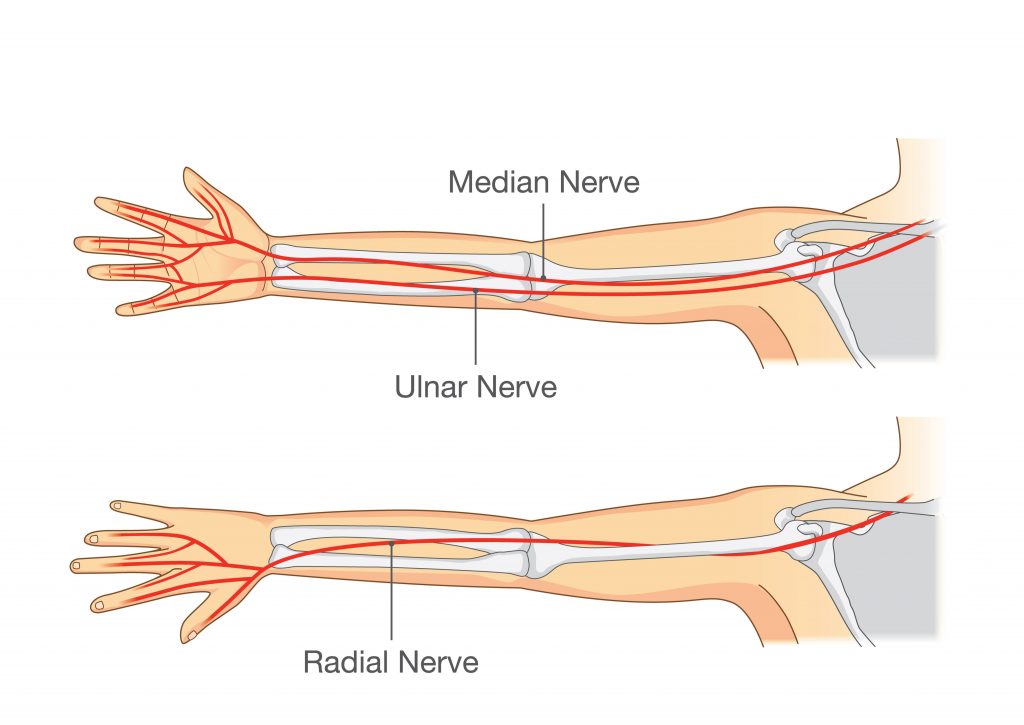
Your ulnar nerve travels along the inner side of your arm down to your hand.
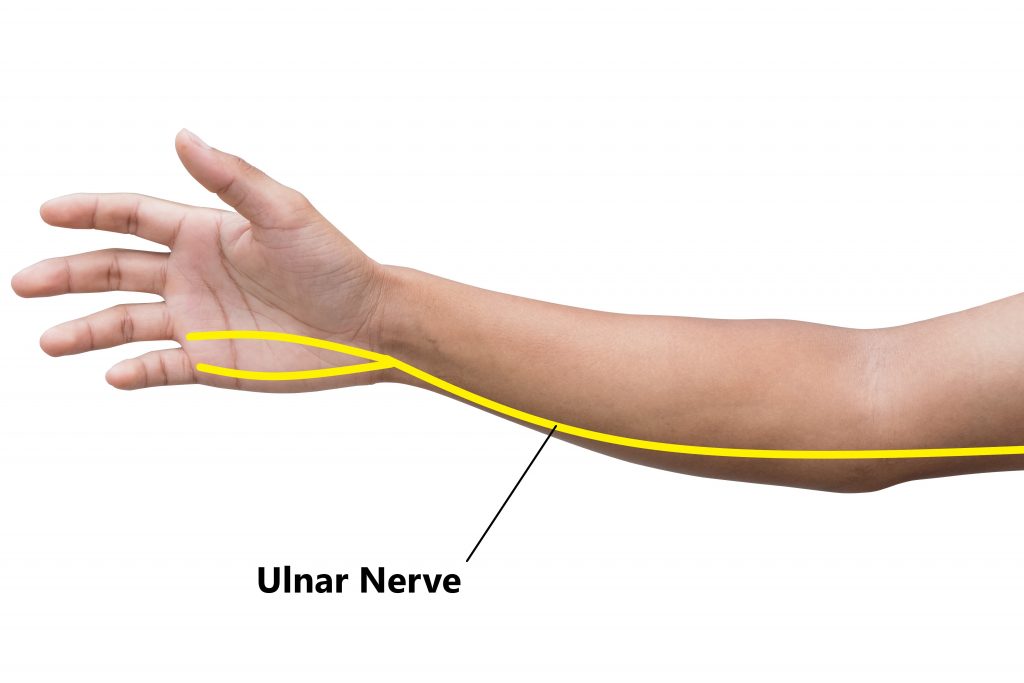
It supplies the muscles in your forearm and hand which enable you to bend your ring and little fingers.

It also supplies the skin on the front and back surfaces of your ring and little fingers to allow sensation.

What is the Cubital Tunnel?
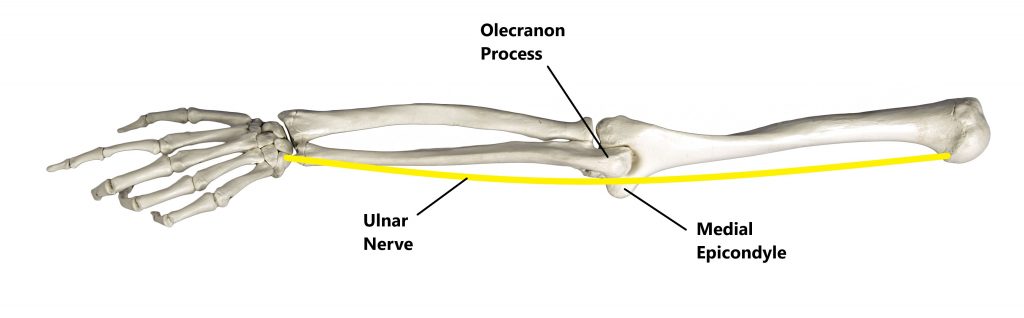
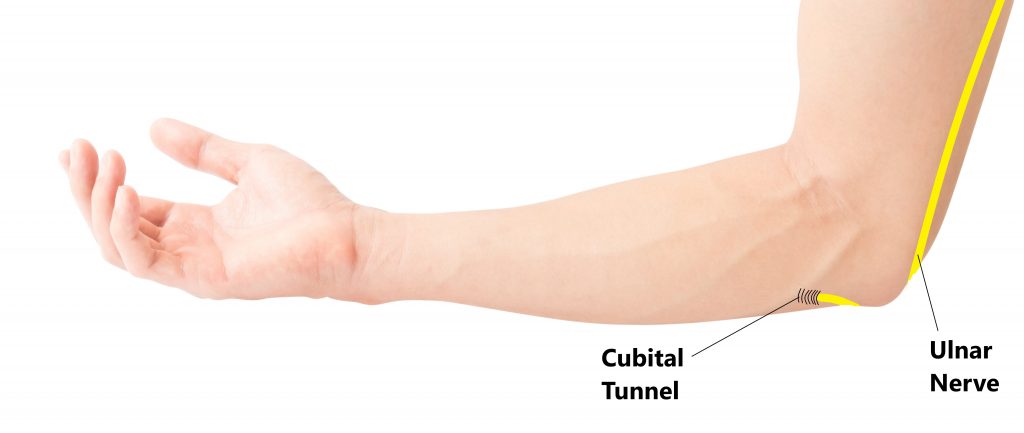
Your ulnar nerve travels between the two prominent bony lumps along the inside of your elbow. This is commonly referred to as the “funny bone” area.
It then passes underneath an inflexible sheath of fibrous tissue, this is known as the cubital tunnel.
What is Cubital Tunnel Syndrome?
This refers to irritation and entrapment of the ulnar nerve as it passes through the inside of the elbow. This can result in symptoms along the inside of the elbow, ring and little finger. There are several sites where this can occur however, the most common is compression of the nerve as it passes through the cubital tunnel.

Common Symptoms
- numbness and tingling in the ring finger and little finger
- pain along the inside of the elbow and forearm
- irritation of symptoms when the elbow is held in a bent position for a prolonged period of time (i.e. using a mobilie phone, driving, sleeping)
- irritation of symptoms following repeated throwing motions
- a flicking sensation over the inside of your elbow as it is bent and straightened
- the feeling of your ring finger or little finger “falling asleep”
- difficulty using your hand to manipulate objects especially with tasks requiring a high level of finger dexterity (i.e typing, playing an instrument)
- hand weakness and difficulty gripping
- wasting of the muscles in the hand can occur in chronic long standing cases

Common Causes
- holding prolonged bent elbow positions
- prolonged/repeated leaning on your elbow
- following impact (i.e. hitting the inside of your elbow)
- instability of the ulnar nerve as the elbow is bent and straightened (giving rise to a flicking sensation as the elbow is bent and straightened)
- repeated throwing motions (i.e. baseball, tennis)
- trauma to the elbow (i.e. fractures, ligament strain)
- joint inflammation
- formation of bone spurs or cysts around the elbow joint

Risk Factors
- participating in throwing sports
- trauma to the elbow joint (i.e fracutes)
- occupations involving prolonged/repeated bending at the elbow
- > 40 years of age
- arthritis
- diabetes

Diagnosis
Diagnosing this condition is based on an individual’s clinical presentation through a thorough subjective and physical examination. A nerve conduction study or an EMG may also be required to see how well the nerve is working. An X-Ray may also be required to exclude/identify other injuries (i.e. bone spurs).
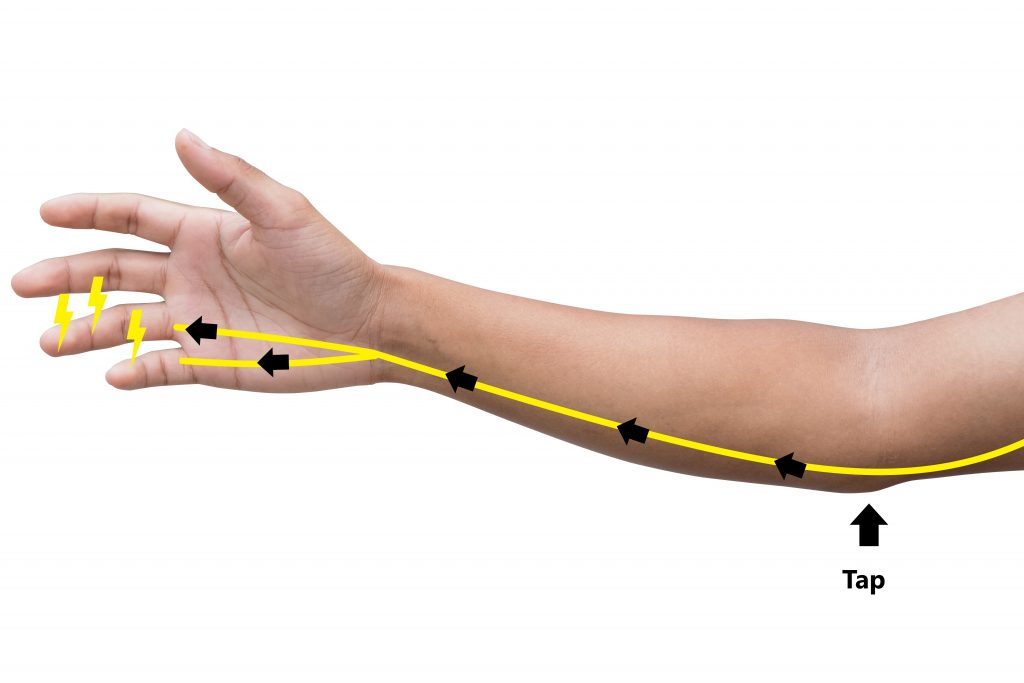
1. With your elbow slightly bent, tap your finger over the ulnar nerve between the olecranon and epicondyle
2. A reproduction of symptoms can be suggestive of cubital tunnel syndrome
Management
Most cases will resolve with conservative treatment, this includes physiotherapy treatment, anti-inflammatory medications and activity modification. More persistent cases may require a cortisone injection. In rare circumstances surgical intervention may be indicated especially when there is progressive weakness and muscle wasting in the hand or clawing of the ring and little finger.

Physiotherapy Management
- Reduce inflammation and decrease pain. Modalities such as RICE (Rest, Ice, Compression, Elevation), splinting and manual therapy may be used.

- Provide education, address unhelpful beliefs regarding the injury, identify and modify aggravating factors (i.e. minimise leaning on elbows and prolonged bent elbow positions)

- Restore pain free wrist range of motion

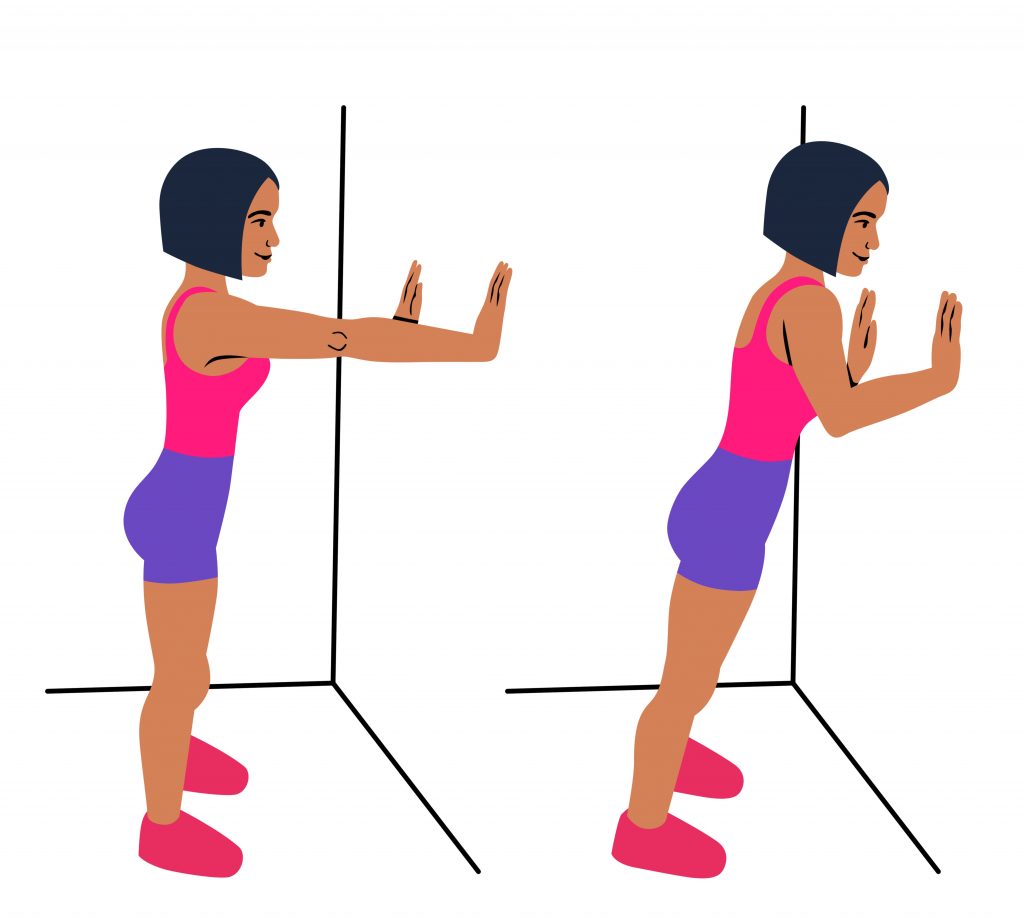
- Restore nerve flexibility

- Strengthen the muscles of the wrist, upper limb and scapula
- Identify and address movement and postural issues that may have contributed to the injury (i.e. stooped posture, poor positioning of the shoulder blades)

Please keep in mind the information provided is general in nature and should not be used as a substitute to consult your treating health professional. If you have any specific questions or require assistance with your individual treatment requirements please do not hesitate to contact My Family Physio in Pittwater Place Shopping Center, Mona Vale.
Related Articles